

Management of therapeutic anticoagulation in patients with intracerebral haemorrhage and mechanical heart valves
- PMID: 29529259
- PMCID: PMC5950928
- DOI: 10.1093/eurheartj/ehy056
Management of therapeutic anticoagulation in patients with intracerebral haemorrhage and mechanical heart valves
Abstract
Aims: Evidence is lacking regarding acute anticoagulation management in patients after intracerebral haemorrhage (ICH) with implanted mechanical heart valves (MHVs). Our objective was to investigate anticoagulation reversal and resumption strategies by evaluating incidences of haemorrhagic and thromboembolic complications, thereby defining an optimal time-window when to restart therapeutic anticoagulation (TA) in patients with MHV and ICH.
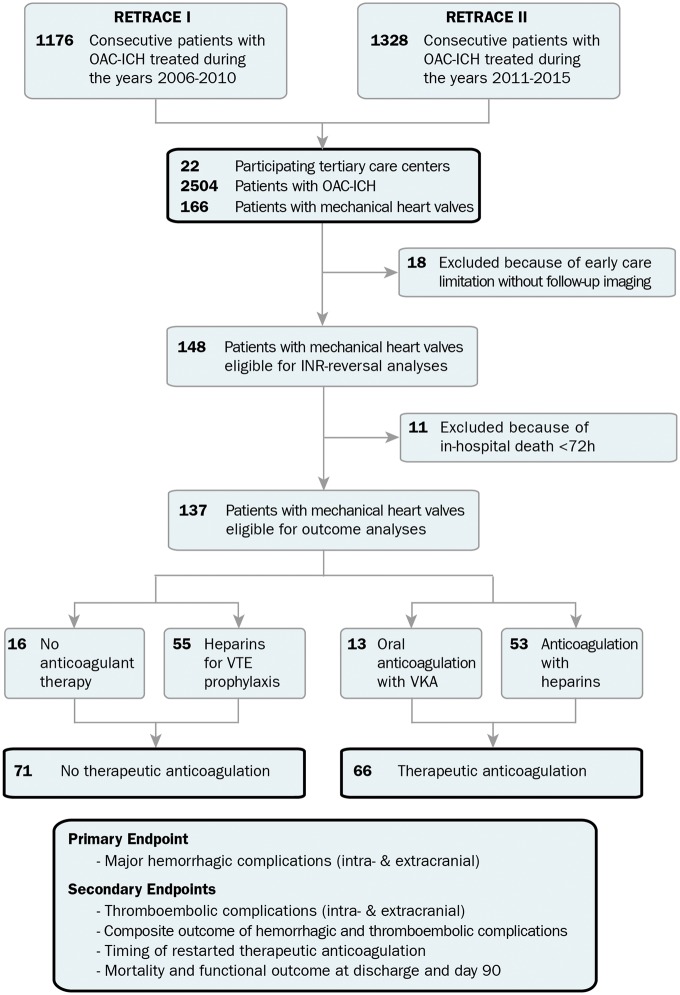
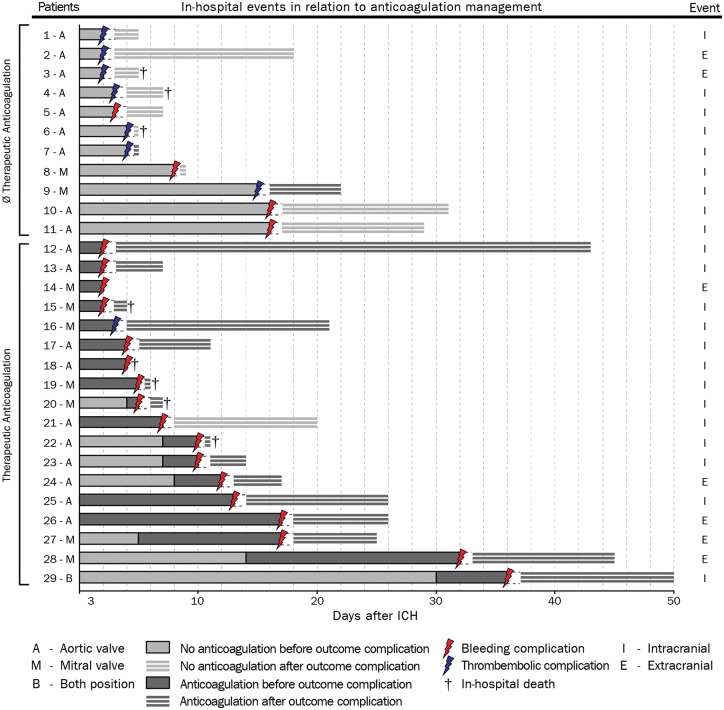
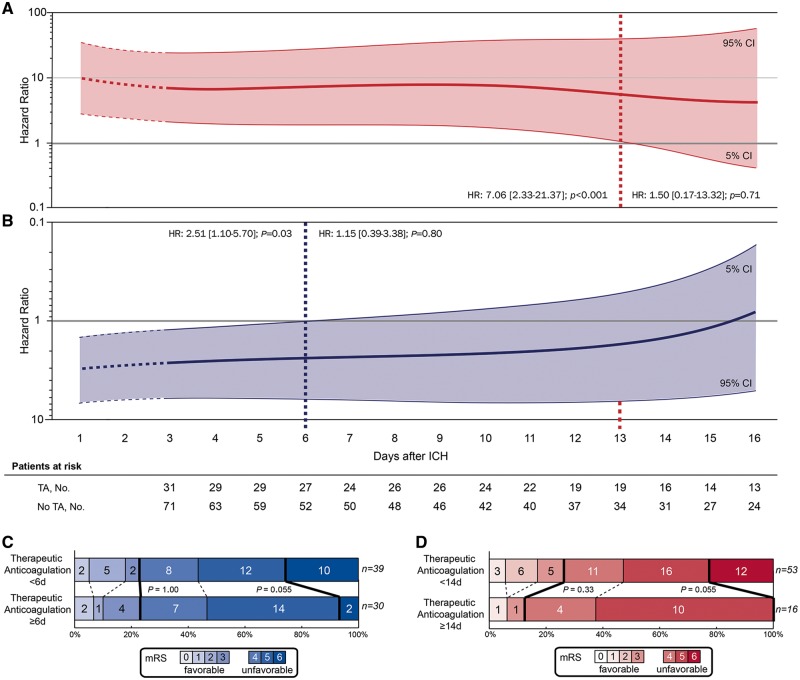
Methods and results: We pooled individual patient-data (n = 2504) from a nationwide multicentre cohort-study (RETRACE, conducted at 22 German centres) and eventually identified MHV-patients (n = 137) with anticoagulation-associated ICH for outcome analyses. The primary outcome consisted of major haemorrhagic complications analysed during hospital stay according to treatment exposure (restarted TA vs. no-TA). Secondary outcomes comprised thromboembolic complications, the composite outcome (haemorrhagic and thromboembolic complications), timing of TA, and mortality. Adjusted analyses involved propensity-score matching and multivariable cox-regressions to identify optimal timing of TA. In 66/137 (48%) of patients TA was restarted, being associated with increased haemorrhagic (TA = 17/66 (26%) vs. no-TA = 4/71 (6%); P < 0.01) and a trend to decreased thromboembolic complications (TA = 1/66 (2%) vs. no-TA = 7/71 (10%); P = 0.06). Controlling treatment crossovers provided an incidence rate-ratio [hazard ratio (HR) 10.31, 95% confidence interval (CI) 3.67-35.70; P < 0.01] in disadvantage of TA for haemorrhagic complications. Analyses of TA-timing displayed significant harm until Day 13 after ICH (HR 7.06, 95% CI 2.33-21.37; P < 0.01). The hazard for the composite-balancing both complications, was increased for restarted TA until Day 6 (HR 2.51, 95% CI 1.10-5.70; P = 0.03).
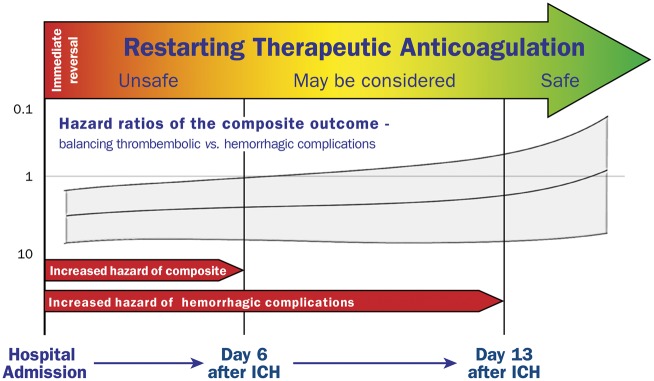
Conclusion: Restarting TA within less than 2 weeks after ICH in patients with MHV was associated with increased haemorrhagic complications. Optimal weighing-between least risks for thromboembolic and haemorrhagic complications-provided an earliest starting point of TA at Day 6, reserved only for patients at high thromboembolic risk.
Figures
Comment in
-
Anticoagulation resumption after intracranial haemorrhage with mechanical valves: a data-free zone.Eur Heart J. 2018 May 14;39(19):1724-1725. doi: 10.1093/eurheartj/ehy116. Eur Heart J. 2018. PMID: 29538640 No abstract available.
References
-
- Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, Iung B, Lancellotti P, Lansac E, Rodriguez Munoz D, Rosenhek R, Sjogren J, Tornos Mas P, Vahanian A, Walther T, Wendler O, Windecker S, Zamorano JL; ESC Scientific Document Group. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J 2017;38:2739–2791. - PubMed
-
- Head SJ, Celik M, Kappetein AP.. Mechanical versus bioprosthetic aortic valve replacement. Eur Heart J 2017;38:2183–2191. - PubMed
-
- Iung B, Rodes-Cabau J.. The optimal management of anti-thrombotic therapy after valve replacement: certainties and uncertainties. Eur Heart J 2014;35:2942–2949. - PubMed
-
- Alfieri O, Vahanian A.. The year in cardiology 2016: valvular heart disease. Eur Heart J 2017;38:628–633. - PubMed
-
- Kuramatsu JB, Gerner ST, Schellinger PD, Glahn J, Endres M, Sobesky J, Flechsenhar J, Neugebauer H, Juttler E, Grau A, Palm F, Rother J, Michels P, Hamann GF, Huwel J, Hagemann G, Barber B, Terborg C, Trostdorf F, Bazner H, Roth A, Wohrle J, Keller M, Schwarz M, Reimann G, Volkmann J, Mullges W, Kraft P, Classen J, Hobohm C, Horn M, Milewski A, Reichmann H, Schneider H, Schimmel E, Fink GR, Dohmen C, Stetefeld H, Witte O, Gunther A, Neumann-Haefelin T, Racs AE, Nueckel M, Erbguth F, Kloska SP, Dorfler A, Kohrmann M, Schwab S, Huttner HB.. Anticoagulant reversal, blood pressure levels, and anticoagulant resumption in patients with anticoagulation-related intracerebral hemorrhage. JAMA 2015;313:824–836. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
