

Prognostic Significance of Large Airway Dimensions on Computed Tomography in the General Population. The Multi-Ethnic Study of Atherosclerosis (MESA) Lung Study
- PMID: 29529382
- PMCID: PMC6137677
- DOI: 10.1513/AnnalsATS.201710-820OC
Prognostic Significance of Large Airway Dimensions on Computed Tomography in the General Population. The Multi-Ethnic Study of Atherosclerosis (MESA) Lung Study
Abstract
Rationale: Large airway dimensions on computed tomography (CT) have been associated with lung function, symptoms, and exacerbations in chronic obstructive pulmonary disease (COPD), as well as with symptoms in smokers with preserved spirometry. Their prognostic significance in persons without lung disease remains undefined.
Objectives: To examine associations between large airway dimensions on CT and respiratory outcomes in a population-based cohort of adults without prevalent lung disease.
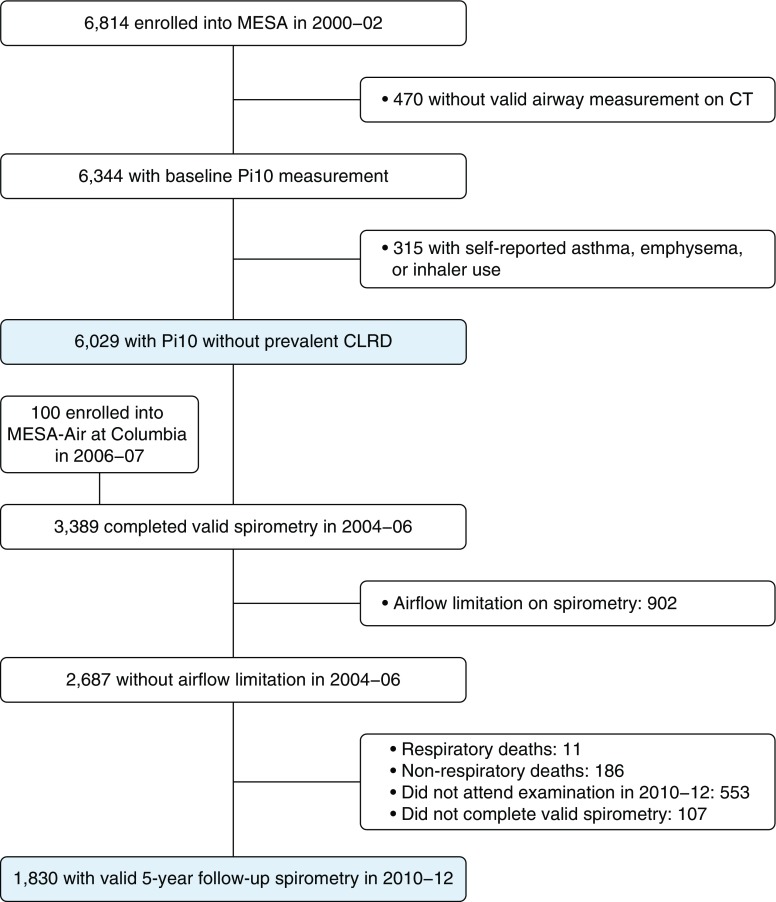
Methods: The Multi-Ethnic Study of Atherosclerosis recruited participants ages 45-84 years without cardiovascular disease in 2000-2002; we excluded participants with prevalent chronic lower respiratory disease (CLRD). Spirometry was measured in 2004-2006 and 2010-2012. CLRD hospitalizations and deaths were classified by validated criteria through 2014. The average wall thickness for a hypothetical airway of 10-mm lumen perimeter on CT (Pi10) was calculated using measures of airway wall thickness and lumen diameter. Models were adjusted for age, sex, principal components of ancestry, body mass index, smoking, pack-years, scanner, percent emphysema, genetic risk score, and initial forced expiratory volume in 1 second (FEV1) percent predicted.
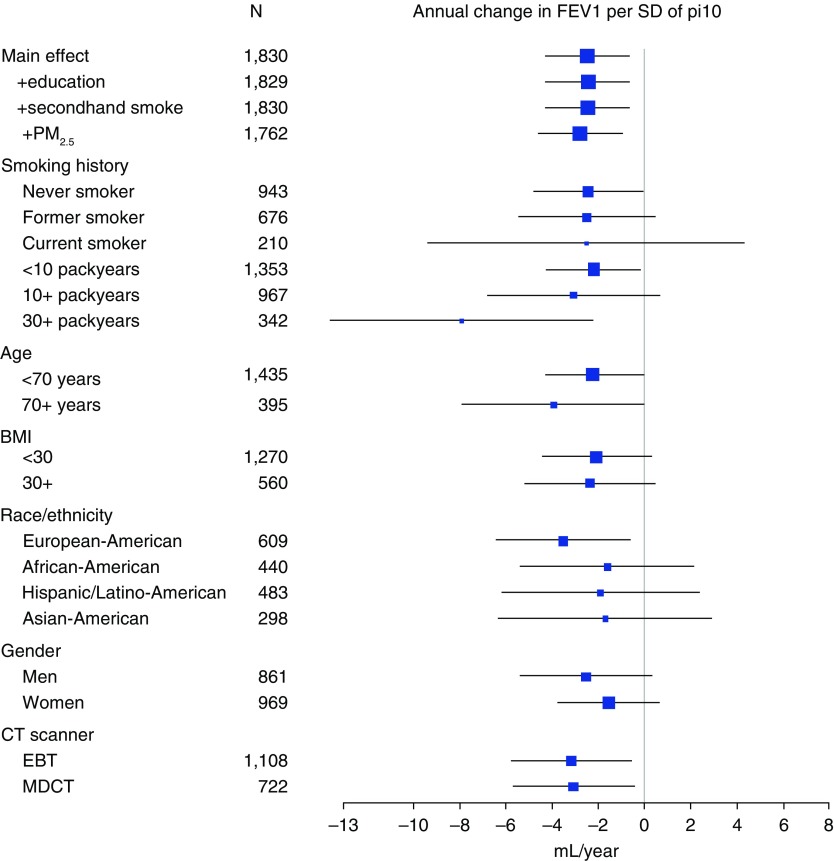
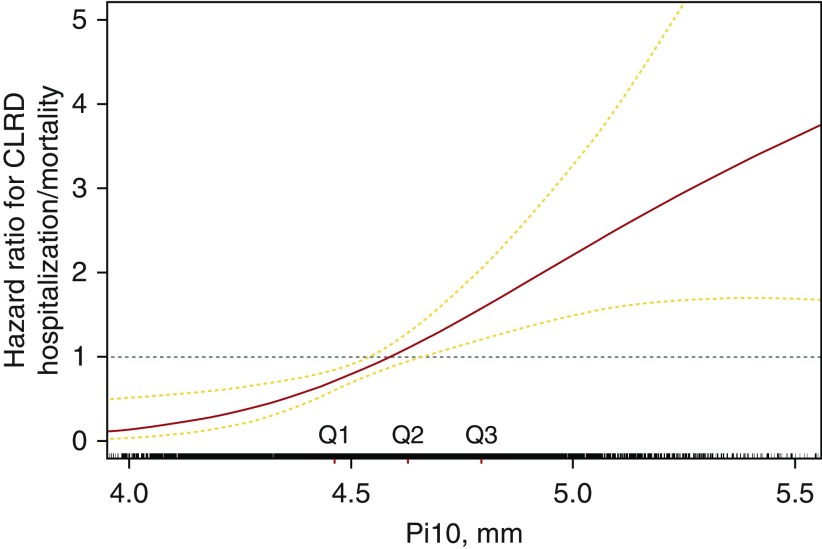
Results: Greater Pi10 was associated with 9% faster FEV1 decline (95% confidence interval [CI], 2 to 15%; P = 0.012) and increased incident COPD (odds ratio, 2.22; 95% CI, 1.43-3.45; P = 0.0004) per standard deviation among 1,830 participants. Over 78,147 person-years, higher Pi10 was associated with a 57% higher risk of first CLRD hospitalization or mortality (P = 0.0496) per standard deviation. Of Pi10's component measures, both greater airway wall thickness and narrower lumen predicted incident COPD and CLRD clinical events.
Conclusions: In adults without CLRD, large airway dimensions on CT were prospectively associated with accelerated lung function decline and increased risks of COPD and CLRD hospitalization and mortality.
Keywords: chronic obstructive pulmonary disease; computed tomography; lung function; risk stratification.
Figures
Comment in
-
Who Is at Risk? The Role of Airway Imaging in Chronic Lung Disease Risk Assessment.Ann Am Thorac Soc. 2018 Jun;15(6):669-670. doi: 10.1513/AnnalsATS.201804-244ED. Ann Am Thorac Soc. 2018. PMID: 29856248 No abstract available.
Similar articles
-
Association of Dysanapsis With Chronic Obstructive Pulmonary Disease Among Older Adults.JAMA. 2020 Jun 9;323(22):2268-2280. doi: 10.1001/jama.2020.6918. JAMA. 2020. PMID: 32515814 Free PMC article.
-
Sex Differences in Airways at Chest CT: Results from the COPDGene Cohort.Radiology. 2022 Dec;305(3):699-708. doi: 10.1148/radiol.212985. Epub 2022 Aug 2. Radiology. 2022. PMID: 35916677 Free PMC article.
-
Occupational Exposures and Computed Tomographic Imaging Characteristics in the SPIROMICS Cohort.Ann Am Thorac Soc. 2018 Dec;15(12):1411-1419. doi: 10.1513/AnnalsATS.201802-150OC. Ann Am Thorac Soc. 2018. PMID: 30339479 Free PMC article.
-
A Genetic Risk Score Associated with Chronic Obstructive Pulmonary Disease Susceptibility and Lung Structure on Computed Tomography.Am J Respir Crit Care Med. 2019 Sep 15;200(6):721-731. doi: 10.1164/rccm.201812-2355OC. Am J Respir Crit Care Med. 2019. PMID: 30925230 Free PMC article.
-
Quantitative computed tomography measurements to evaluate airway disease in chronic obstructive pulmonary disease: Relationship to physiological measurements, clinical index and visual assessment of airway disease.Eur J Radiol. 2016 Nov;85(11):2144-2151. doi: 10.1016/j.ejrad.2016.09.010. Epub 2016 Sep 13. Eur J Radiol. 2016. PMID: 27776670 Free PMC article. Review.
Cited by
-
Lung function decline in former smokers and low-intensity current smokers: a secondary data analysis of the NHLBI Pooled Cohorts Study.Lancet Respir Med. 2020 Jan;8(1):34-44. doi: 10.1016/S2213-2600(19)30276-0. Epub 2019 Oct 9. Lancet Respir Med. 2020. PMID: 31606435 Free PMC article.
-
Quantitative Assessment of Airway Changes in Fibrotic Interstitial Lung Abnormality Patients by Chest CT According to Cumulative Cigarette Smoking.Tomography. 2022 Apr 3;8(2):1024-1032. doi: 10.3390/tomography8020082. Tomography. 2022. PMID: 35448716 Free PMC article.
-
Computed tomography total airway count predicts progression to COPD in at-risk smokers.ERJ Open Res. 2021 Oct 25;7(4):00307-2021. doi: 10.1183/23120541.00307-2021. eCollection 2021 Oct. ERJ Open Res. 2021. PMID: 34708120 Free PMC article.
-
Quantitative imaging analysis detects subtle airway abnormalities in symptomatic military deployers.BMC Pulm Med. 2022 Apr 27;22(1):163. doi: 10.1186/s12890-022-01960-w. BMC Pulm Med. 2022. PMID: 35477425 Free PMC article.
-
A Multidimensional Diagnostic Approach for Chronic Obstructive Pulmonary Disease.JAMA. 2025 Jun 24;333(24):2164-2175. doi: 10.1001/jama.2025.7358. JAMA. 2025. PMID: 40382791
References
-
- Kochanek KD, Murphy S, Xu J, Arias E. Mortailty in the United States, 2016. NCHS Data Brief. 2017;293:1–8. - PubMed
Publication types
MeSH terms
Grants and funding
- N01 HC095161/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- R01 HL077612/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- R01 HL093081/HL/NHLBI NIH HHS/United States
- R21 HL129924/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- R01 HL075476/HL/NHLBI NIH HHS/United States
- R01 HL130506/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- P30 ES005605/ES/NIEHS NIH HHS/United States
- R01 HL112986/HL/NHLBI NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- K23 HL130627/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
- P30 ES009089/ES/NIEHS NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
