

Synchronous gastric leiomyoma and intramuscular abdominal wall granular cell tumor with similar imaging features: A case report
- PMID: 29529541
- PMCID: PMC5928285
- DOI: 10.1016/j.ijscr.2018.03.001
Synchronous gastric leiomyoma and intramuscular abdominal wall granular cell tumor with similar imaging features: A case report
Abstract
Introduction: Gastric leiomyomas are benign mesenchymal tumors, comprising about 2.5% of gastric neoplasms, which can be difficult to differentiate from gastrointestinal stromal tumors which have malignant potential. Granular cell tumors in the abdominal wall are also rare. Since mesenchymal tumors are difficult to diagnose by imaging, further studies are needed to establish the diagnosis.
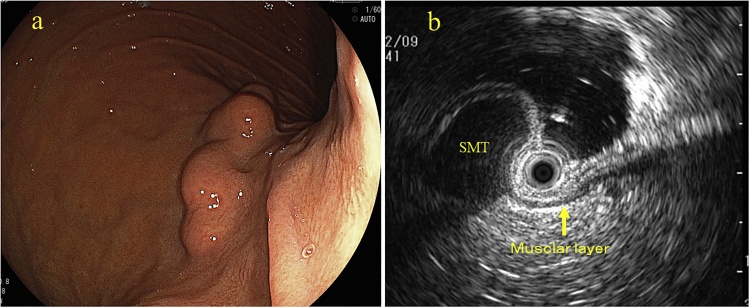
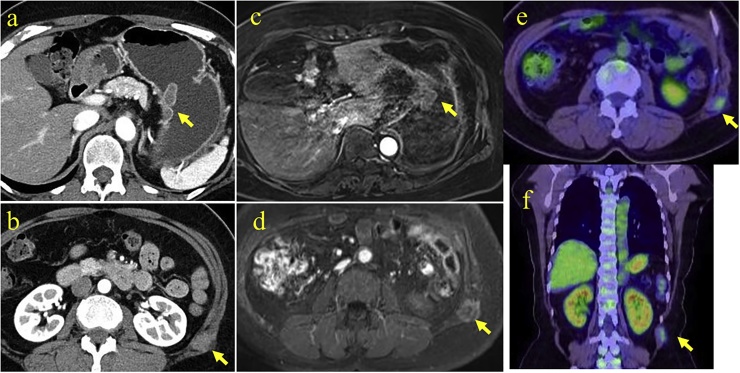
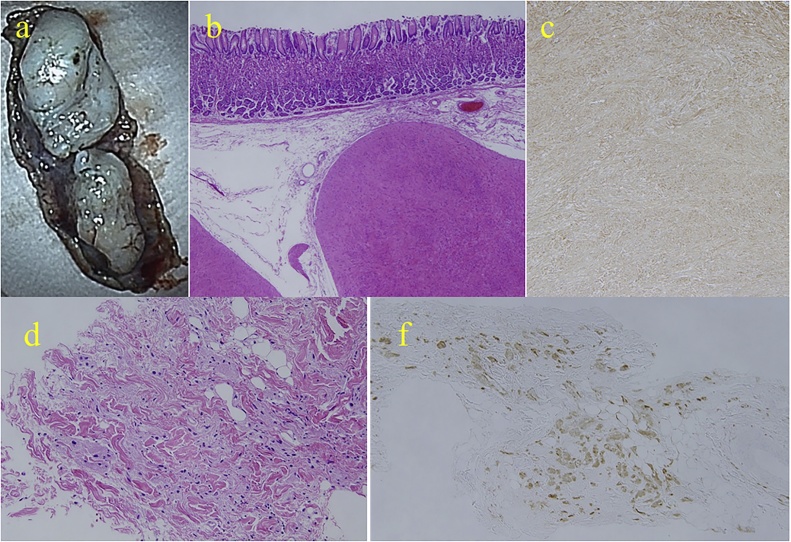
Presentation of case: A 60-year-old asymptomatic woman underwent routine upper endoscopy and was found to have a gastric submucosal lesion. Computed tomography scan also showed an abdominal wall mass. The appearance of both lesions on imaging studies were similar, but it was unclear if the two lesions had the same origin. Endoscopic ultrasound-guided fine needle aspiration biopsy of the gastric lesion was insufficient to establish the diagnosis. Laparoscopic-endoscopic cooperative resection of the gastric lesion and ultrasound-guided core-needle biopsy of the abdominal wall mass enabled pathological diagnosis of both lesions.
Discussion: Diagnostic imaging findings of these two lesions were similar. Histologic and immunohistochemical studies are essential to establish a definitive diagnosis. Laparoscopic-endoscopic cooperative surgery may be an effective minimally invasive approach, allowing both pathological diagnosis and complete resection of a gastric submucosal tumor, especially when endoscopic-ultrasound guided fine needle aspiration or biopsy fails to make the diagnosis.
Conclusion: Laparoscopic-endoscopic cooperative surgery can be an effective minimally invasive approach to resect some lesions. This is first report of the patient with a synchronous gastric leiomyoma and an intramuscular granular cell tumor in the abdominal wall.
Keywords: Case report; Gastric leiomyoma; Granular cell tumor; Laparoscopic-endoscopic cooperative surgery.
Copyright © 2018 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Hirose Y., Kaida H., Kawahara A., Kurata S., Ishibashi M., Abe T. (1)(8)F-FDG PET/CT and contrast enhanced CT in differential diagnosis between leiomyoma and gastrointestinal stromal tumor. Hell J. Nucl. Med. 2015;18(3):257–260. - PubMed
-
- Min Y.W., Park H.N., Min B.H., Choi D., Kim K.M., Kim S. Preoperative predictive factors for gastrointestinal stromal tumors: analysis of 375 surgically resected gastric subepithelial tumors. J. Gastrointest. Surg. 2015;19(4):631–638. - PubMed
-
- Yang H.K., Kim Y.H., Lee Y.J., Park J.H., Kim J.Y., Lee K.H. Leiomyomas in the gastric cardia: CT findings and differentiation from gastrointestinal stromal tumors. Eur. J. Radiol. 2015;84(9):1694–1700. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
