

Otto Aufranc Award: Dual-mobility Constructs in Revision THA Reduced Dislocation, Rerevision, and Reoperation Compared With Large Femoral Heads
- PMID: 29529658
- PMCID: PMC6259708
- DOI: 10.1007/s11999.0000000000000035
Otto Aufranc Award: Dual-mobility Constructs in Revision THA Reduced Dislocation, Rerevision, and Reoperation Compared With Large Femoral Heads
Abstract
Background: Dislocation is one of the most common complications after revision THA. Dual-mobility constructs and large femoral heads (ie, 40 mm) are two contemporary, nonconstrained bearing options used in revision THA to minimize the risk of dislocation; however, it is not currently established if there is a clear benefit to using dual-mobility constructs over large femoral heads in the revision setting.
Questions/purposes: We sought to determine if dual-mobility constructs would provide a reduction in dislocation, rerevision for dislocation, and reoperation or other complications as compared with large femoral heads in revision THA.
Methods: From 2011 to 2014, a series of 355 THAs underwent revision for any reason and received either a dual-mobility construct (146 THAs) or a 40-mm large femoral head (209 THAs). Indications for either construct were based on surgeon judgment; however, there is a preference to use dual-mobility constructs in patients believed to be at higher risk of dislocation. In the dual-mobility group, 20 of 146 (14%) were excluded because of loss of followup before 2 years or because they had a dual-mobility shell cemented into a preexisting acetabular component. In the large head group, 33 of 209 (16%) were lost to followup before 2 years. Followup in the dual-mobility group was 3.3 ± 0.8 years and followup in the large head group was 3.9 ± 0.9 years. Primary endpoints included dislocation, rerevisions for dislocation, and reoperations, which were determined through our institution's total joint registry and verified by individual patient chart review. Age and body mass index were not different with the numbers available between the groups, but there was a slight predominance of females in the dual-mobility group (52% [66 of 126] female) versus the 40-mm large head group (41% [72 of 176] female) (p = 0.05). Notably, 33% (41 of 126) of patients receiving the dual-mobility constructs had the index revision THA done for a diagnosis of recurrent dislocation versus 9% (17 of 176) in the 40-mm large head group. Mean effective head size in the dual-mobility group was 47 mm (range, 38-58 mm).
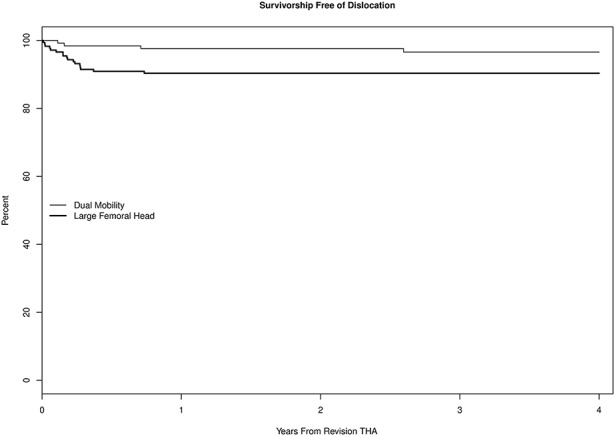
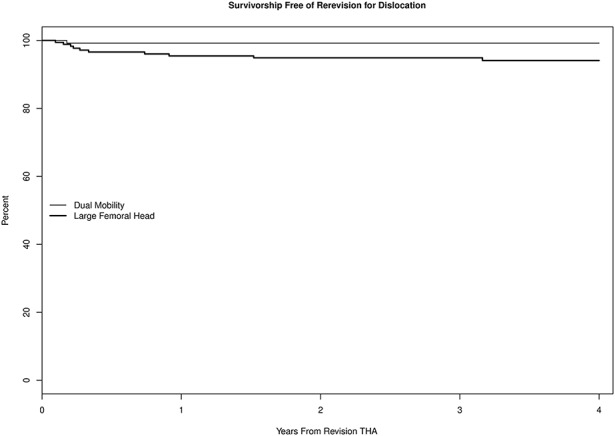
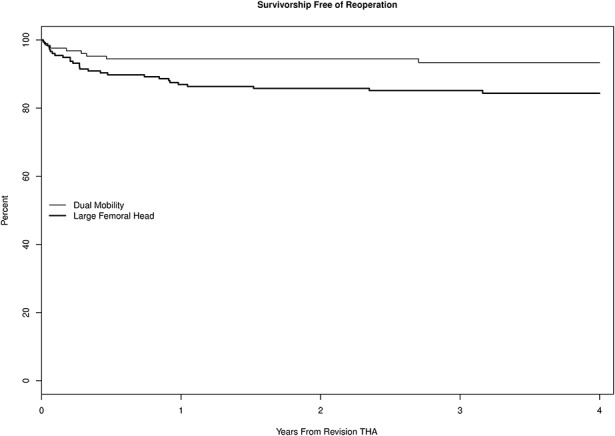
Results: The subsequent frequency of dislocation in the dual-mobility construct group was less (3% [four of 126] dual-mobility versus 10% [17 of 176] in the 40-mm large head group; hazard ratio, 3.2 [1.1-9.4]; p = 0.03). Rerevision for dislocation in the dual-mobility construct group was less frequent (1% [one of 126] dual-mobility versus 6% [10 of 176] in the 40-mm large head group; hazard ratio, 7.1 [0.9-55.6]; p = 0.03). Reoperation for any cause in the dual-mobility construct group was less frequent (6% [eight of 126] dual-mobility versus 15% [27 of 176] in the 40-mm large head group; hazard ratio, 2.5 [1.1-5.5]; p = 0.02); there were no differences between the groups in terms of the overall percentage of complications in each group.
Conclusions: When compared with patients treated with a 40-mm large femoral head, patients undergoing revision THA who received a dual-mobility construct had a lower risk of subsequent dislocation, rerevision for dislocation, and reoperation for any reason in the first several years postoperatively. Those findings were present despite selection bias in this study to use the dual-mobility construct in patients at the highest risk for subsequent dislocation. Given the lower risk of subsequent dislocation, rerevision, and reoperation with the dual-mobility construct, some surgeons may wish to consider whether the role of dual-mobility should be judiciously expanded in contemporary revision THA.
Level of evidence: Level III, therapeutic study.
Conflict of interest statement
All ICMJE Conflict of Interest Forms for authors and
Figures
Comment in
-
CORR Insights®: Otto Aufranc Award: Dual-mobility Constructs in Revision THA Reduced Dislocation, Rerevision, and Reoperation Compared With Large Femoral Heads.Clin Orthop Relat Res. 2018 Feb;476(2):302-304. doi: 10.1007/s11999.0000000000000120. Clin Orthop Relat Res. 2018. PMID: 29529659 Free PMC article. No abstract available.
Similar articles
-
In Revision THA, Is the Re-revision Risk for Dislocation and Aseptic Causes Greater in Dual-mobility Constructs or Large Femoral Head Bearings? A Study from the Australian Orthopaedic Association National Joint Replacement Registry.Clin Orthop Relat Res. 2022 Jun 1;480(6):1091-1101. doi: 10.1097/CORR.0000000000002085. Epub 2022 Jan 3. Clin Orthop Relat Res. 2022. PMID: 34978538 Free PMC article.
-
Can Dislocation of a Constrained Liner Be Salvaged With Dual-mobility Constructs in Revision THA?Clin Orthop Relat Res. 2018 Feb;476(2):305-312. doi: 10.1007/s11999.0000000000000026. Clin Orthop Relat Res. 2018. PMID: 29529660 Free PMC article.
-
Is There a Difference in Revision Risk Between Metal and Ceramic Heads on Highly Crosslinked Polyethylene Liners?Clin Orthop Relat Res. 2017 May;475(5):1349-1355. doi: 10.1007/s11999-016-4966-1. Clin Orthop Relat Res. 2017. PMID: 27385222 Free PMC article.
-
Dissociation and Intrapelvic Entrapment of a Dual-mobility Polyethylene Component.Clin Orthop Relat Res. 2016 Apr;474(4):1072-6. doi: 10.1007/s11999-015-4381-z. Epub 2015 Jun 19. Clin Orthop Relat Res. 2016. PMID: 26088765 Free PMC article. Review.
-
Dual-Mobility Constructs in Primary and Revision Total Hip Arthroplasty: A Systematic Review of Comparative Studies.J Arthroplasty. 2019 Mar;34(3):594-603. doi: 10.1016/j.arth.2018.11.020. Epub 2018 Nov 17. J Arthroplasty. 2019. PMID: 30554926
Cited by
-
Risk factors and modes of failure in the modern dual mobility implant. A systematic review and meta-analysis.BMC Musculoskelet Disord. 2021 Jun 14;22(1):541. doi: 10.1186/s12891-021-04404-4. BMC Musculoskelet Disord. 2021. PMID: 34126990 Free PMC article.
-
Dual-mobility cups in revision acetabular reconstructions: Short-term outcomes in high-risk patients for instability.Acta Orthop Traumatol Turc. 2019 Sep;53(5):329-333. doi: 10.1016/j.aott.2019.05.002. Epub 2019 Jul 4. Acta Orthop Traumatol Turc. 2019. PMID: 31281078 Free PMC article.
-
Dual mobility cups reduce dislocation in isolated cup revision.BMC Musculoskelet Disord. 2025 Mar 29;26(1):308. doi: 10.1186/s12891-025-08553-8. BMC Musculoskelet Disord. 2025. PMID: 40155895 Free PMC article.
-
Unstable Total Hip Arthroplasty: Should It Be Revised Using Dual Mobility Implants? A Retrospective Analysis from the R.I.P.O. Registry.J Clin Med. 2023 Jan 5;12(2):440. doi: 10.3390/jcm12020440. J Clin Med. 2023. PMID: 36675369 Free PMC article.
-
Dislocated and Dissociated Dual-Mobility Components Are Easily Missed and More Than Half Fail Closed Reduction: Six Tips to Aid Management.JB JS Open Access. 2023 Jul 17;8(3):e22.00108. doi: 10.2106/JBJS.OA.22.00108. eCollection 2023 Jul-Sep. JB JS Open Access. 2023. PMID: 37461408 Free PMC article.
References
-
- Berry DJ. Unstable total hip arthroplasty: detailed overview. Instr Course Lect. 2001;50:265–274. - PubMed
-
- Carter AH, Sheehan EC, Mortazavi SM, Purtill JJ, Sharkey PF, Parvizi J. Revision for recurrent instability: what are the predictors of failure? J Arthroplasty. 2011;26(Suppl):46–52. - PubMed
-
- Chang RW, Pellisier JM, Hazen GB. A cost-effectiveness analysis of total hip arthroplasty for osteoarthritis of the hip. JAMA. 1996;275:858–865. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
