

Time to diagnosis and associated costs of an outpatient vs inpatient setting in the diagnosis of lymphoma: a retrospective study of a large cohort of major lymphoma subtypes in Spain
- PMID: 29530002
- PMCID: PMC5848556
- DOI: 10.1186/s12885-018-4187-y
Time to diagnosis and associated costs of an outpatient vs inpatient setting in the diagnosis of lymphoma: a retrospective study of a large cohort of major lymphoma subtypes in Spain
Abstract
Background: Mainly because of the diversity of clinical presentations, diagnostic delays in lymphoma can be excessive. The time spent in primary care before referral to the specialist may be relatively short compared with the interval between hospital appointment and diagnosis. Although studies have examined the diagnostic intervals and referral patterns of patients with lymphoma, the time to diagnosis of outpatient compared to inpatient settings and the costs incurred are unknown.
Methods: We performed a retrospective study at two academic hospitals to evaluate the time to diagnosis and associated costs of hospital-based outpatient diagnostic clinics or conventional hospitalization in four representative lymphoma subtypes. The frequency, clinical and prognostic features of each lymphoma subtype and the activities of the two settings were analyzed. The costs incurred during the evaluation were compared by microcosting analysis.
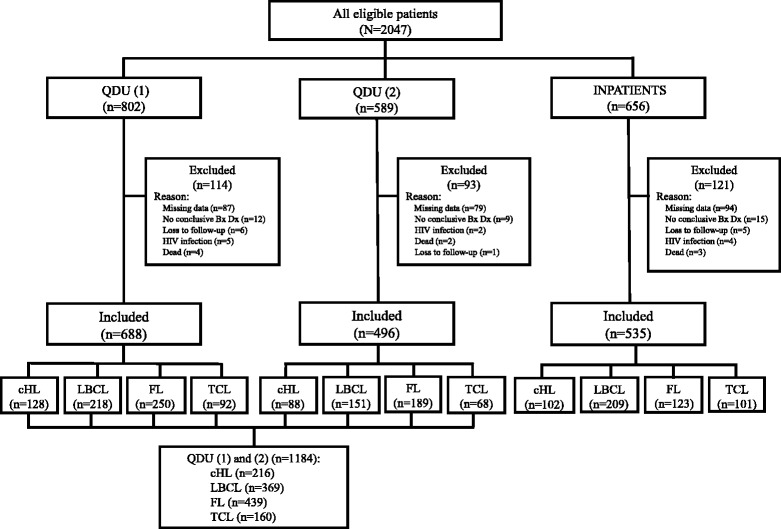
Results: A total of 1779 patients diagnosed between 2006 and 2016 with classical Hodgkin, large B-cell, follicular, and mature nodal peripheral T-cell lymphomas were identified. Clinically aggressive subtypes including large B-cell and peripheral T-cell lymphomas were more commonly diagnosed in inpatients than in outpatients (39.1 vs 31.2% and 18.9 vs 13.5%, respectively). For each lymphoma subtype, inpatients were older and more likely than outpatients to have systemic symptoms, worse performance status, more advanced Ann Arbor stages, and high-risk prognostic scores. The admission time for diagnosis (i.e. from admission to excisional biopsy) of inpatients was significantly shorter than the time to diagnosis of outpatients (12.3 [3.3] vs 16.2 [2.7] days; P < .001). Microcosting revealed a mean cost of €4039.56 (513.02) per inpatient and of €1408.48 (197.32) per outpatient, or a difference of €2631.08 per patient.
Conclusions: Although diagnosis of lymphoma was quicker with hospitalization, the outpatient approach seems to be cost-effective and not detrimental. Despite the considerable savings with the latter approach, there may be hospitalization-associated factors which may not be properly managed in an outpatient unit (e.g. aggressive lymphomas with severe symptoms) and the cost analysis did not account for this potentially added value. While outcomes were not analyzed in this study, the impact on patient outcome of an outpatient vs inpatient diagnostic setting may represent a challenging future research.
Keywords: Diagnosis; Emergency departments; Excisional biopsy; Fine-needle aspiration cytology; Inpatient; Length of stay; Lymphoma; Outpatient; Primary care; Time to diagnosis.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Comitè d’ Ètica de la Investigació Clínica (Clinical Research Ethics Committee) of the Hospital Clínic and the Comitè d’ Ètica i Assajos Clínics (Ethics and Clinical Assays Committee) of the University Hospital of Bellvitge. The ethics committees waived the need for written informed consent because no intervention was involved and the retrospective analysis of clinical data.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
