

Mechanisms of implementing public health interventions: a pooled causal mediation analysis of randomised trials
- PMID: 29530060
- PMCID: PMC5848564
- DOI: 10.1186/s13012-018-0734-9
Mechanisms of implementing public health interventions: a pooled causal mediation analysis of randomised trials
Abstract
Background: The World Health Organization recommends that nations implement evidence-based nutritional guidelines and policies in settings such as schools and childcare services to improve public health nutrition. Understanding the causal mechanism by which implementation strategies exert their effects could enhance guideline implementation. The aim of this study was to assess the mechanisms by which implementation strategies improved schools and childcare services' adherence to nutrition guidelines.
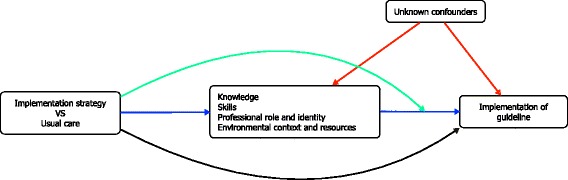
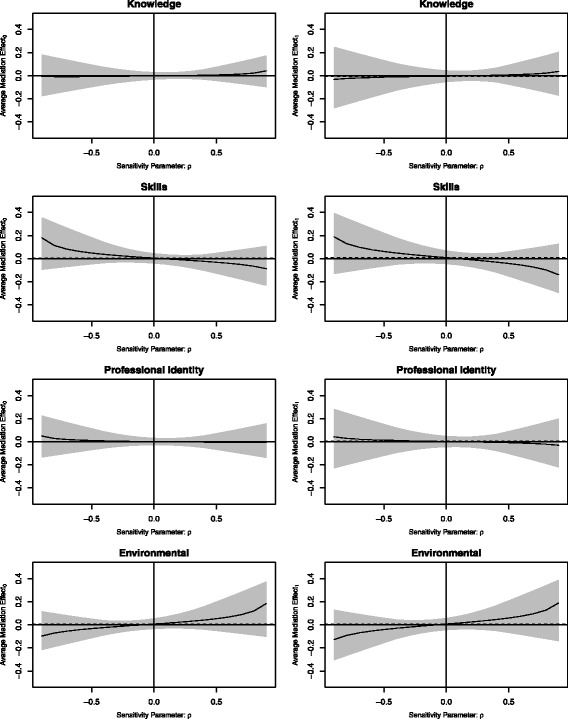
Methods: We conducted a mechanism evaluation of an aggregated dataset generated from three randomised controlled trials conducted in schools and childcare services in New South Wales, Australia. Each trial examined the impact of implementation strategies that targeted Theoretical Domains Framework constructs including knowledge, skills, professional role and identity, environmental context and resources. We pooled aggregated organisation level data from each trial, including quantitative assessments of the Theoretical Domains Framework constructs, as well as measures of school or childcare nutrition guideline compliance, the primary implementation outcome. We used causal mediation analysis to estimate the average indirect and direct effects of the implementation strategies and assessed the robustness of our findings to varying levels of unmeasured and unknown confounding.
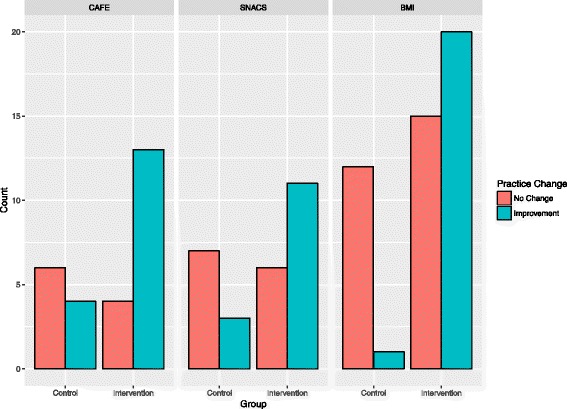
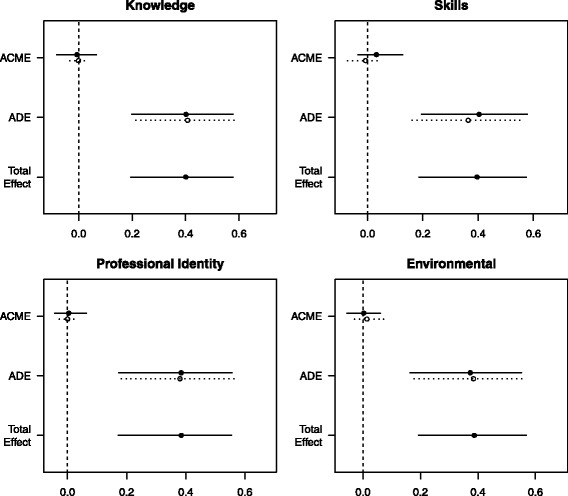
Results: We included 121 schools or childcare services in the pooled analysis: 79 allocated to receive guideline and policy implementation strategies and 42 to usual practice. Overall, the interventions improved compliance (odds ratio = 6.64; 95% CI [2.58 to 19.09]); however, the intervention effect was not mediated by any of the four targeted Theoretical Domains Framework constructs (average causal mediation effects through knowledge = - 0.00 [- 0.05 to 0.04], skills = 0.01 [- 0.02 to 0.07], professional role and identity = 0.00 [- 0.03 to 0.03] and environmental context and resources = 0.00 [- 0.02 to 0.06]). The intervention had no significant effect on the four targeted Theoretical Domains Framework constructs, and the constructs were not associated with school or childcare nutrition guideline compliance. Potentially, this lack of effect could be explained by imprecise measurement of the mediators. Alternatively, it is likely that that the interventions were operating via alternative mechanisms that were not captured by the four Theoretical Domains Framework constructs we explored.
Conclusions: Even though public health implementation strategies led to meaningful improvements in school or childcare nutrition guideline compliance, these effects were not mediated by key targeted constructs of the Theoretical Domains Framework. Future research should explore the mechanistic role of other Theoretical Domains Framework constructs and evaluate system-level mechanisms informed by an ecological framework.
Trial registration: All trials were prospectively registered with the Australian New Zealand Clinical Trials Registry ( ACTRN12613000543785 . Registered 15/05/2013; ACTRN12614001148662 . Registered 30/10/2014; ACTRN12615001032549 . Registered 1/10/2015).
Keywords: Implementation science; Mechanism; Mediation analysis; Public health; Theoretical domains framework.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval to conduct this study was obtained from Hunter New England Human Research Ethics Committee (ref. no. 06/07/26/4.04), University of Newcastle (ref. no. H-2008-0343) and New South Wales (NSW) Department of Education (SERAP 2012277).
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet [Internet] 2012;380:2224–2260. doi: 10.1016/S0140-6736(12)61766-8. - DOI - PMC - PubMed
-
- World Health Organization. General Assembly proclaims the Decade of Action on Nutrition [Internet]. 2016. Available from: http://www.who.int/nutrition/GA_decade_action/en/. Accessed 3 Nov 2017.
-
- NHMRC. Australian Dietary Guidelines [Internet]. Natl Heal Med Res Counc. 2013. Available from: www.nhmrc.gov.au/guidelines-publications/n55. Accessed 3 Nov 2017.
-
- World Health Organization. Ambition and Action in Nutrition 2016-2025 [Internet]. 2017. Available from: http://www.who.int/nutrition/publications/nutrition-strategy-2016to2025/en/. Accessed 3 Nov 2017.
-
- NSW Department of Health, NSW Department of Education and Training. Fresh Tastes @ School NSW healthy school canteen strategy: canteen menu planning guide. 3rd ed. Sydney: NSW Department of Health, NSW Department of Education and Training; 2012.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
