

Technology-assisted title and abstract screening for systematic reviews: a retrospective evaluation of the Abstrackr machine learning tool
- PMID: 29530097
- PMCID: PMC5848519
- DOI: 10.1186/s13643-018-0707-8
Technology-assisted title and abstract screening for systematic reviews: a retrospective evaluation of the Abstrackr machine learning tool
Abstract
Background: Machine learning tools can expedite systematic review (SR) processes by semi-automating citation screening. Abstrackr semi-automates citation screening by predicting relevant records. We evaluated its performance for four screening projects.
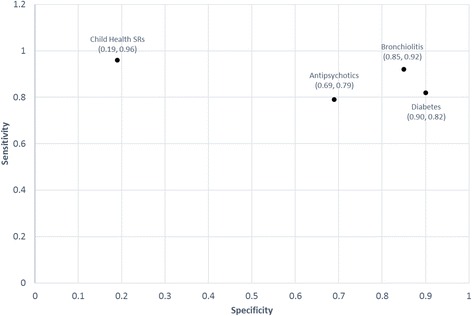
Methods: We used a convenience sample of screening projects completed at the Alberta Research Centre for Health Evidence, Edmonton, Canada: three SRs and one descriptive analysis for which we had used SR screening methods. The projects were heterogeneous with respect to search yield (median 9328; range 5243 to 47,385 records; interquartile range (IQR) 15,688 records), topic (Antipsychotics, Bronchiolitis, Diabetes, Child Health SRs), and screening complexity. We uploaded the records to Abstrackr and screened until it made predictions about the relevance of the remaining records. Across three trials for each project, we compared the predictions to human reviewer decisions and calculated the sensitivity, specificity, precision, false negative rate, proportion missed, and workload savings.
Results: Abstrackr's sensitivity was > 0.75 for all projects and the mean specificity ranged from 0.69 to 0.90 with the exception of Child Health SRs, for which it was 0.19. The precision (proportion of records correctly predicted as relevant) varied by screening task (median 26.6%; range 14.8 to 64.7%; IQR 29.7%). The median false negative rate (proportion of records incorrectly predicted as irrelevant) was 12.6% (range 3.5 to 21.2%; IQR 12.3%). The workload savings were often large (median 67.2%, range 9.5 to 88.4%; IQR 23.9%). The proportion missed (proportion of records predicted as irrelevant that were included in the final report, out of the total number predicted as irrelevant) was 0.1% for all SRs and 6.4% for the descriptive analysis. This equated to 4.2% (range 0 to 12.2%; IQR 7.8%) of the records in the final reports.
Conclusions: Abstrackr's reliability and the workload savings varied by screening task. Workload savings came at the expense of potentially missing relevant records. How this might affect the results and conclusions of SRs needs to be evaluated. Studies evaluating Abstrackr as the second reviewer in a pair would be of interest to determine if concerns for reliability would diminish. Further evaluations of Abstrackr's performance and usability will inform its refinement and practical utility.
Keywords: Automation; Machine learning; Methodology; Systematic review.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- JPT H, Green S, editors. Cochrane handbook for systematic reviews of interventions. 2011.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
