

Monitoring the effect of first line treatment in RAS/RAF mutated metastatic colorectal cancer by serial analysis of tumor specific DNA in plasma
- PMID: 29530101
- PMCID: PMC5848434
- DOI: 10.1186/s13046-018-0723-5
Monitoring the effect of first line treatment in RAS/RAF mutated metastatic colorectal cancer by serial analysis of tumor specific DNA in plasma
Abstract
Background: Precision medicine calls for an early indicator of treatment efficiency. Circulating tumor DNA (ctDNA) is a promising marker in this setting. Our prospective study explored the association between disease development and change of ctDNA during first line chemotherapy in patients with RAS/RAF mutated metastatic colorectal cancer (mCRC).
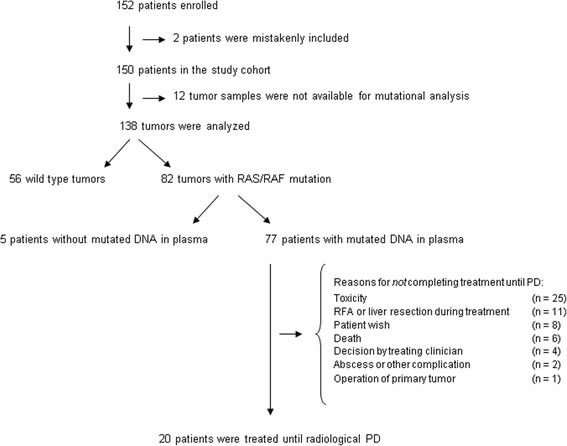
Methods: The study included 138 patients with mCRC receiving standard first line treatment. In patients with RAS/RAF mutated tumor DNA the same mutation was quantified in the plasma using droplet digital PCR. The fractional abundance of ctDNA was assessed in plasma before treatment start and at every treatment cycle until radiologically defined progressive disease.
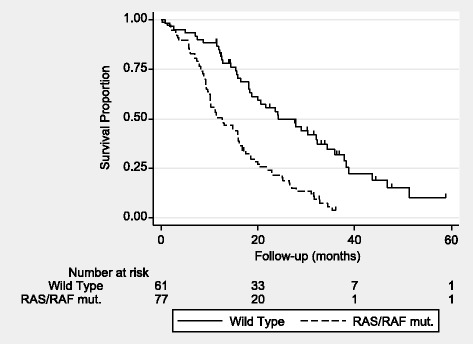
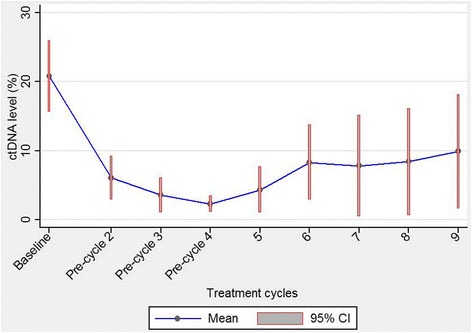
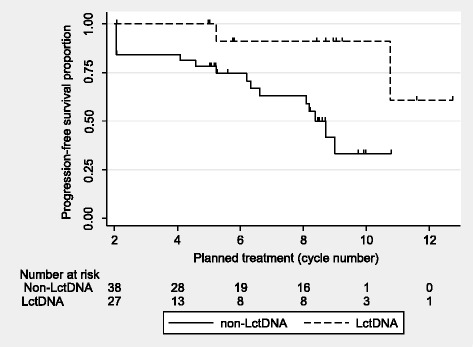
Results: RAS/RAF mutations were detected in the plasma from 77 patients. Twenty patients progressed on treatment and 57 stopped treatment without progression. The presence of mutated DNA in plasma was correlated with poor overall survival. A low level of ctDNA after the first cycle of chemotherapy was associated with a low risk of progression. On the other hand, a significant increase of ctDNA at any time during the treatment course was associated with a high risk of progression on continuous treatment. The first increase in ctDNA level occurred at a median of 51 days before radiologically confirmed progression.
Conclusions: The results indicate that the ctDNA level holds potential as a clinically valuable marker in first line treatment of mCRC. A rapid decrease was associated with a prolonged progression free interval, whereas a significant increase gave notice of early progression with a relevant lead time.
Keywords: Circulating tumor DNA; Liquid biopsy; Metastatic colorectal cancer; Monitoring; RAS/RAF mutations; Treatment efficiency.
Conflict of interest statement
Ethics approval and consent to participate
All patients gave oral and written consent to participate in the study. The study was approved by The Regional Committees on Health Research Ethics for Southern Denmark (S-20100005) and the investigation was conducted in accordance with the REMARK criteria [12].
Consent for publication
Not applicable.
Competing interests
The authors have declared no conflicts of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Maughan TS, Adams RA, Smith CG, et al. Addition of cetuximab to oxaliplatin-based first-line combination chemotherapy for treatment of advanced colorectal cancer: results of the randomised phase 3 MRC COIN trial. Lancet. 2011;377(9783):2103–2114. doi: 10.1016/S0140-6736(11)60613-2. - DOI - PMC - PubMed
-
- Thierry AR, El Messaoudi S, Mollevi C, et al. Clinical utility of circulating DNA analysis for rapid detection of actionable mutations to select metastatic colorectal patients for anti-EGFR treatment. Ann Oncol. 2017;28:2149–59. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
