

Contemporary Burn Survival
- PMID: 29530306
- PMCID: PMC6027619
- DOI: 10.1016/j.jamcollsurg.2017.12.045
Contemporary Burn Survival
Abstract
Background: The standard of burn treatment today reflects major advances. We sought to quantitate the impact of these advances on burn survival via age-stratified mortality ratios compared with other reported mortality analyses in burns.
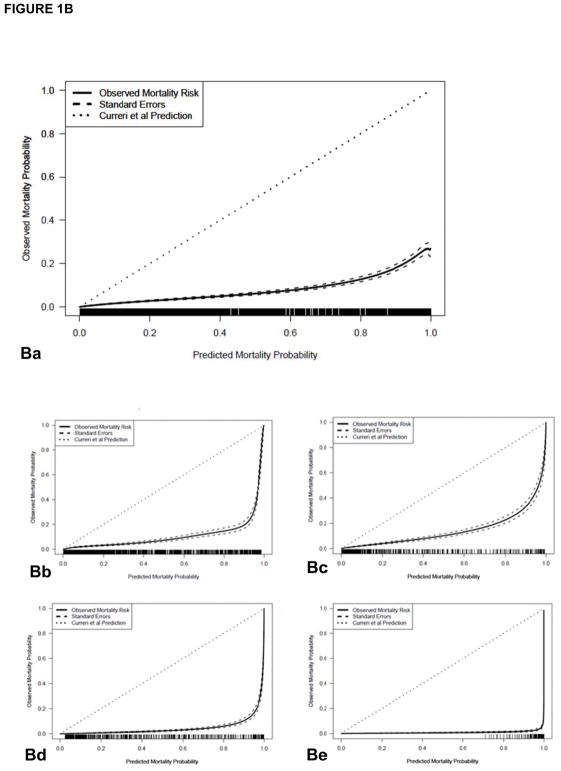
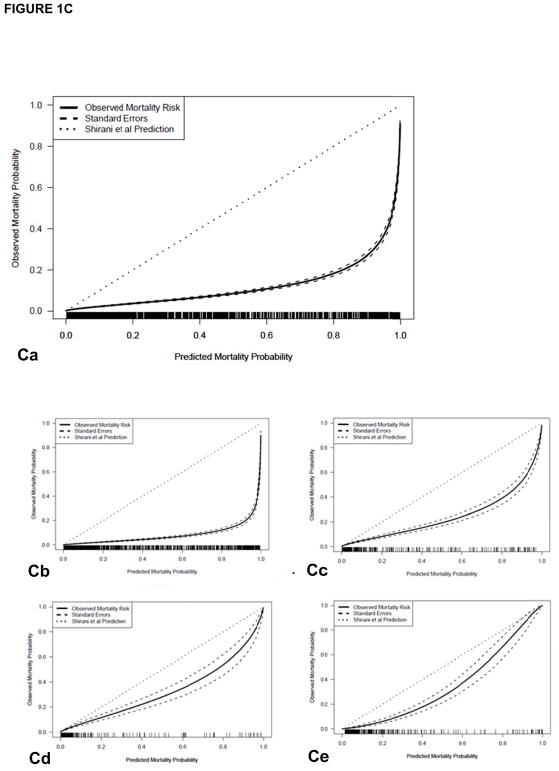
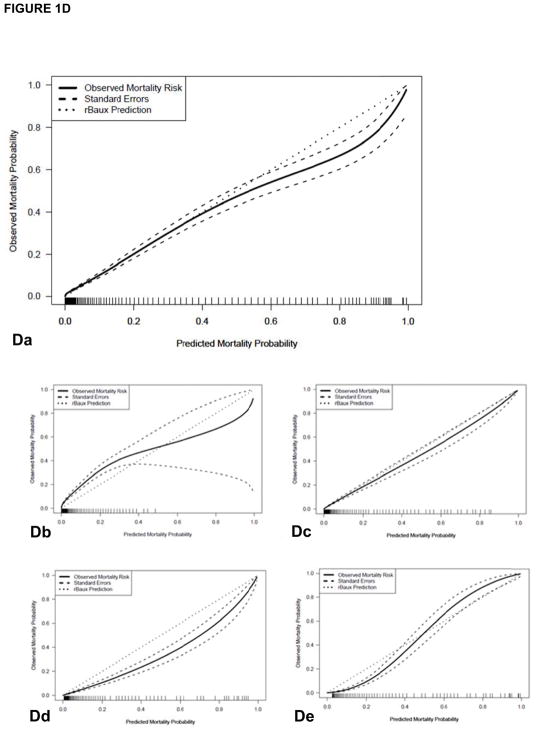
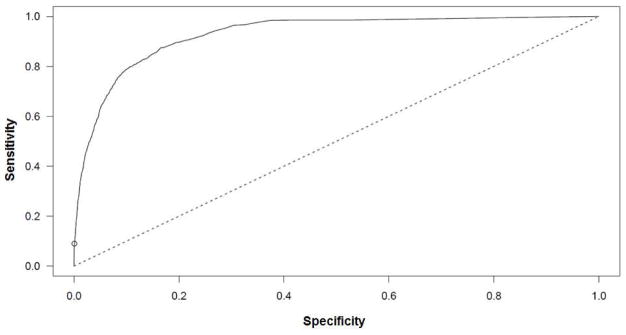
Study design: Age, percent of the total body surface area (TBSA) burned, presence of inhalation injury, length of stay, and survival status were recorded at admission and at discharge for all new burn admissions between 1989 and 2017. The expected mortality probability was calculated using historical multiple regression techniques and compared with observed data. We developed a prediction model for our observed data.
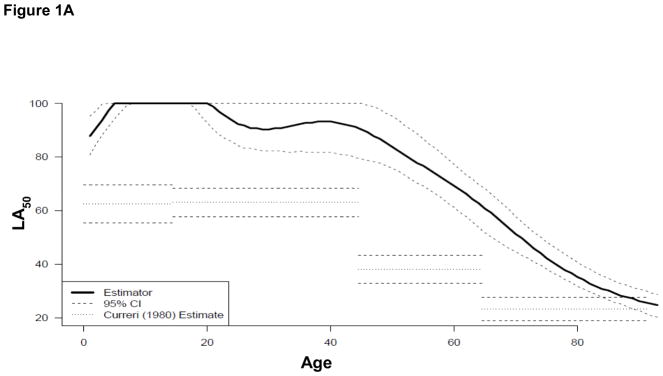
Results: Between 1989 and 2017, there were 10,384 consecutive new burn admissions, with 355 mortalities (median age, 13 years; median percent TBSA burn, 11%). We saw a significant decrease in our observed mortality data compared to historical predictions (p < 0.0001), and a 2% reduction per year in mortality during the 3 decades. The prediction model of mortality for the data is as follows: Pr(dying) = ex/(1 + ex) where x = -6.44 - 0.12 age + 0.0042 age2 - 0.0000283 age3 + 0.0499 TBSA + 1.21 Inhalation Injury + 0.015 third degree TBSA.
Conclusions: The reduction in mortality over time may be attributed to successful changes in standard of care protocols in the burn center that improved the outlook for burned individuals, including protocols for management of inhalation injury, nutrition, resuscitation, and early excision and grafting.
Copyright © 2018. Published by Elsevier Inc.
Figures
Comment in
-
Discussion.J Am Coll Surg. 2018 Apr;226(4):463-464. doi: 10.1016/j.jamcollsurg.2018.01.031. J Am Coll Surg. 2018. PMID: 29576147 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
