

Effectiveness of a community-based educational programme in reducing the cumulative incidence and prevalence of human Taenia solium cysticercosis in Burkina Faso in 2011-14 (EFECAB): a cluster-randomised controlled trial
- PMID: 29530423
- PMCID: PMC5873982
- DOI: 10.1016/S2214-109X(18)30027-5
Effectiveness of a community-based educational programme in reducing the cumulative incidence and prevalence of human Taenia solium cysticercosis in Burkina Faso in 2011-14 (EFECAB): a cluster-randomised controlled trial
Abstract
Background: The effectiveness of drug-free interventions in controlling human cysticercosis is not well known. We aimed to estimate the effectiveness of a community-based educational intervention in reducing the frequency of human cysticercosis in Burkina Faso.
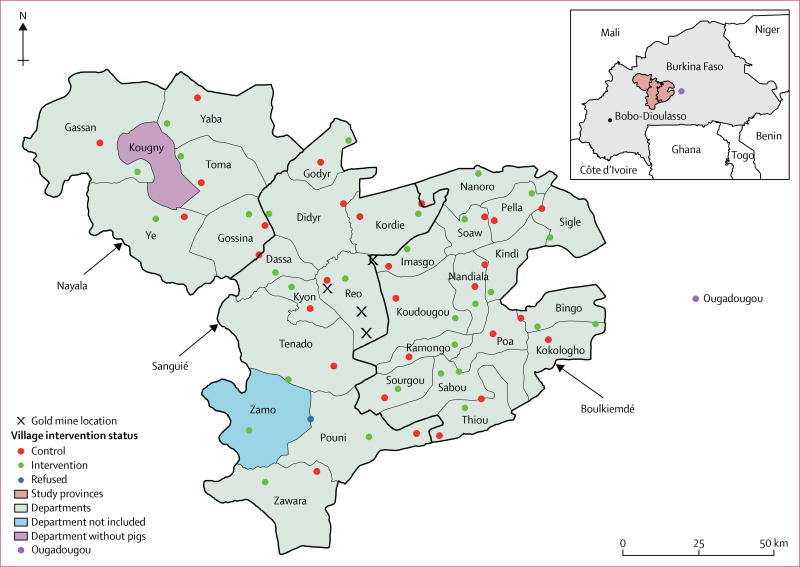
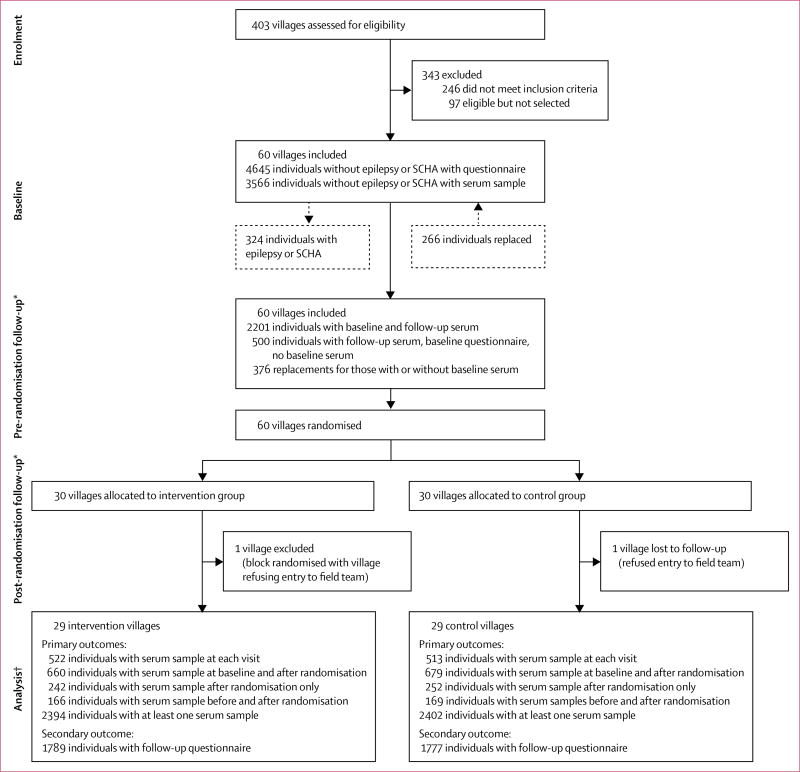
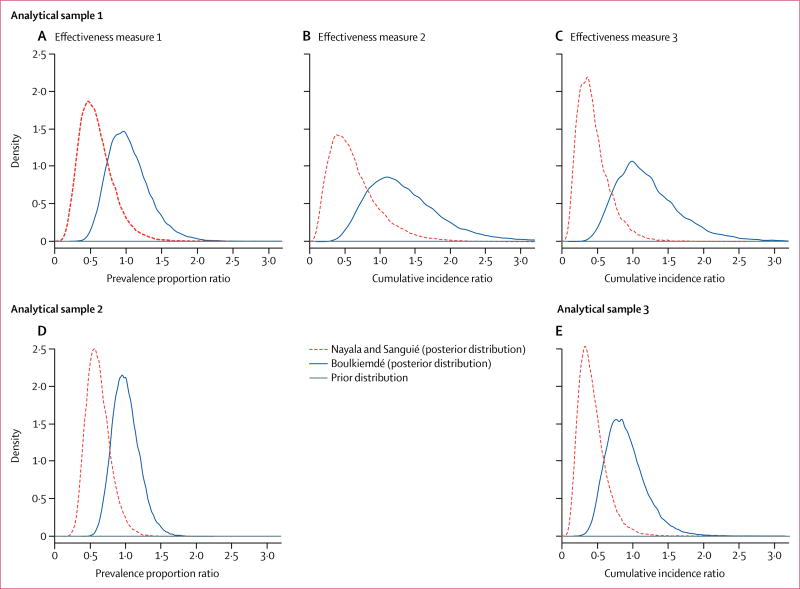
Methods: We did a cluster-randomised controlled trial between 2011 and 2014. 60 eligible villages from three provinces (Boulkiemdé, Sanguié, and Nayala) were randomly allocated to the intervention or control group. Villages raising pigs, that were not a regional capital or located on a main road, that were more than 20 km from Ouagadougou or 5 km from one another, were eligible. In each village, 60 participants were asked for blood samples at baseline, 18 months later (before randomisation), and 18 months after randomisation. Villages were block randomised (1:1) by pig-raising department immediately after the pre-randomisation visit. The intervention aimed to improve knowledge of Taenia solium transmission and control through screening and structured discussion of a 52-min movie, and to increase community self-efficacy through a Self-esteem, Associative strengths, Resourcefulness, Action planning, Responsibility (SARAR) approach via the Participatory Hygiene and Sanitation Transformation (PHAST) model. The primary outcome was active cysticercosis, defined as the presence of circulating antigens detected by use of B158/B60 ELISA. Effectiveness measured at the village level was estimated by use of three Bayesian hierarchical models. This study is registered with ClinicalTrials.gov, number NCT0309339.
Findings: Two villages in the same randomisation block were excluded, resulting in a final sample size of 58 villages. Overall, the intervention tended towards a decrease in the cumulative incidence of active cysticercosis from baseline to after randomisation (adjusted cumulative incidence ratio 0·65, 95% Bayesian credible interval [95% CrI] 0·39-1·05) and a decrease in active cysticercosis prevalence from baseline to after randomisation (adjusted prevalence proportion ratio 0·84; 95% CrI 0·59-1·18). The intervention was shown to be effective in Nayala and Sanguié but not in Boulkiemdé.
Interpretation: Community-engaged participatory interventions can be effective at reducing the incidence and prevalence of cysticercosis in some low-resource settings.
Funding: US National Institutes of Health (National Institute of Neurological Disorders and Stroke, Fogarty International Center, and National Institute of General Medical Sciences).
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
All other authors declare no competing interests.
Figures
Comment in
-
Effectiveness of an education-based control option for human cysticercosis.Lancet Glob Health. 2018 Apr;6(4):e359-e360. doi: 10.1016/S2214-109X(18)30103-7. Lancet Glob Health. 2018. PMID: 29530413 No abstract available.
References
-
- Carabin H, Krecek RC, Cowan LD, et al. Estimation of the cost of Taenia solium cysticercosis in Eastern Cape Province, South Africa. Trop Med Intl Health. 2006;11:906–16. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
