

Association Between 30-Day Episode Payments and Acute Myocardial Infarction Outcomes Among Medicare Beneficiaries
- PMID: 29530887
- PMCID: PMC5922453
- DOI: 10.1161/CIRCOUTCOMES.117.004397
Association Between 30-Day Episode Payments and Acute Myocardial Infarction Outcomes Among Medicare Beneficiaries
Abstract
Background: Recent policy efforts have focused on improving the value of acute myocardial infarction (AMI) care. Medicare payment programs, for example, increasingly evaluate hospital performance based on spending, as determined by payments made to institutions and providers, and outcome measures for a longitudinal episode of AMI care. Little is known about the relationship between total 30-day payments-both in the inpatient and immediate postdischarge timeframe-and outcomes after an admission for AMI.
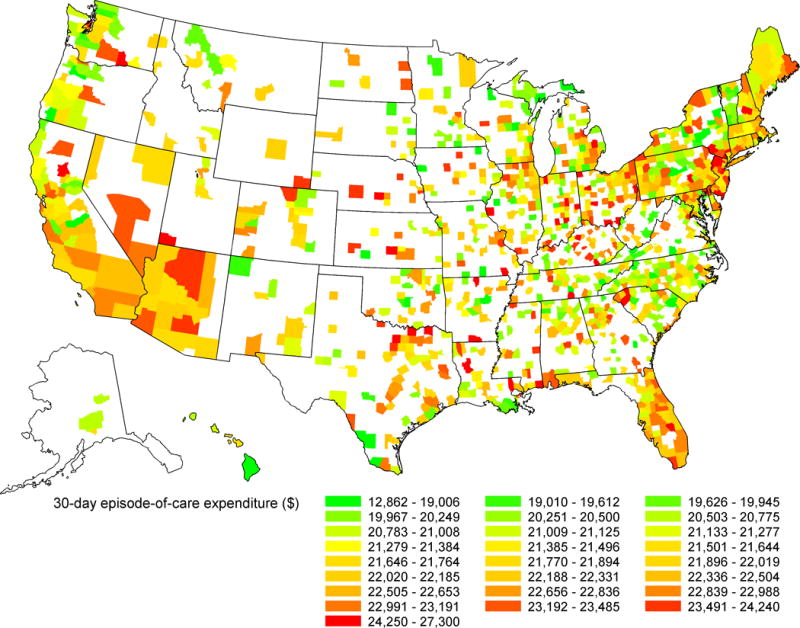
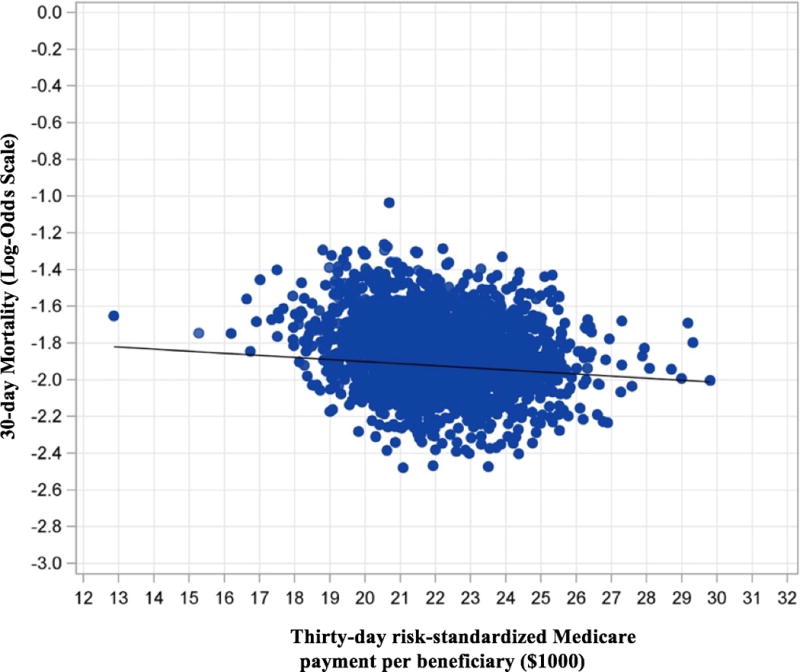
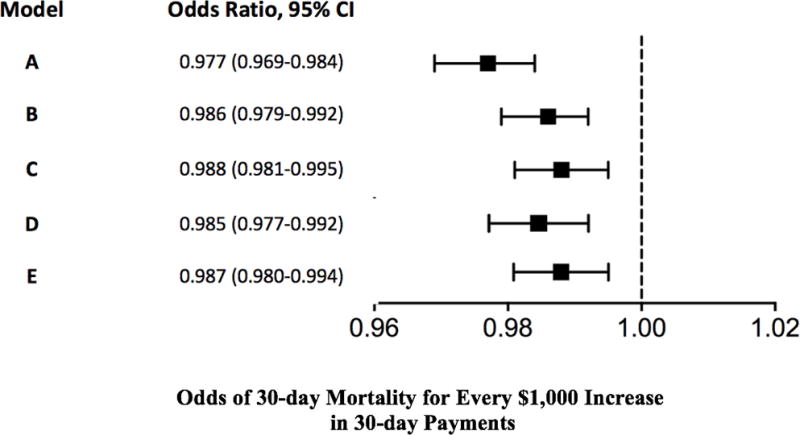
Methods and results: Using Medicare claims data, we identified Medicare fee-for-service beneficiaries ≥65 years of age who were hospitalized at an acute-care hospital for AMI between July 1, 2011, and June 30, 2014, and examined the association between hospital-level 30-day payments for an episode of AMI care and patient 30-day mortality using mixed regression models with a logit link function and random hospital intercepts. Our cohort included 642 105 index hospitalizations for AMI at 2319 acute-care hospitals. Overall mean 30-day episode payments per beneficiary were $22 128 (SD, $1750). The observed 30-day mortality rate was 12.9%. Higher 30-day payments were associated with lower 30-day mortality after adjustment for patient characteristics and comorbidities (adjusted odds ratio for additional $1000 payments, 0.986; 95% confidence interval, 0.979-0.992; P<0.001). Additional adjustment for potential mediating factors, including hospital characteristics, coronary revascularization rates, and discharge disposition, did not significantly attenuate the relationship (adjusted odds ratio for additional $1000 payments, 0.987; 95% confidence interval, 0.980-0.994; P<0.001).
Conclusions: Higher hospital-level 30-day payments-both inpatient and in multiple settings after discharge-for AMI care were associated with lower 30-day mortality among beneficiaries. This may have implications for payment programs that incent reduction in payments without considering value.
Keywords: Medicare; health expenditures; mortality; myocardial infarction; percutaneous coronary intervention.
© 2018 American Heart Association, Inc.
Conflict of interest statement
All other co-authors have no disclosures
Figures
Similar articles
-
The Effect of Medicare Accountable Care Organizations on Early and Late Payments for Cardiovascular Disease Episodes.Circ Cardiovasc Qual Outcomes. 2018 Aug;11(8):e004495. doi: 10.1161/CIRCOUTCOMES.117.004495. Circ Cardiovasc Qual Outcomes. 2018. PMID: 30354375 Free PMC article.
-
Association Between Postoperative Pneumonia and 90-Day Episode Payments and Outcomes Among Medicare Beneficiaries Undergoing Cardiac Surgery.Circ Cardiovasc Qual Outcomes. 2018 Sep;11(9):e004818. doi: 10.1161/CIRCOUTCOMES.118.004818. Circ Cardiovasc Qual Outcomes. 2018. PMID: 30354549
-
30-Day Episode Payments and Heart Failure Outcomes Among Medicare Beneficiaries.JACC Heart Fail. 2018 May;6(5):379-387. doi: 10.1016/j.jchf.2017.11.010. Epub 2018 Apr 11. JACC Heart Fail. 2018. PMID: 29655827 Free PMC article.
-
Medicare in the 21 st Century: Understanding the Program to Promote Improvements.J Am Acad Orthop Surg. 2024 May 15;32(10):427-438. doi: 10.5435/JAAOS-D-23-00464. Epub 2024 Apr 9. J Am Acad Orthop Surg. 2024. PMID: 38595137 Free PMC article. Review.
-
Geographic Adjustment in Medicare Payment: Phase II: Implications for Access, Quality, and Efficiency.Washington (DC): National Academies Press (US); 2011 Jul 17. Washington (DC): National Academies Press (US); 2011 Jul 17. PMID: 24921116 Free Books & Documents. Review.
Cited by
-
Association Between Medicare Expenditures and Adverse Events for Patients With Acute Myocardial Infarction, Heart Failure, or Pneumonia in the United States.JAMA Netw Open. 2020 Apr 1;3(4):e202142. doi: 10.1001/jamanetworkopen.2020.2142. JAMA Netw Open. 2020. PMID: 32259263 Free PMC article.
-
2024 Heart Disease and Stroke Statistics: A Report of US and Global Data From the American Heart Association.Circulation. 2024 Feb 20;149(8):e347-e913. doi: 10.1161/CIR.0000000000001209. Epub 2024 Jan 24. Circulation. 2024. PMID: 38264914 Free PMC article. Review.
-
Incidence, Risk Factors, and Outcomes Associated With In-Hospital Acute Myocardial Infarction.JAMA Netw Open. 2019 Jan 4;2(1):e187348. doi: 10.1001/jamanetworkopen.2018.7348. JAMA Netw Open. 2019. PMID: 30657538 Free PMC article.
-
2025 Heart Disease and Stroke Statistics: A Report of US and Global Data From the American Heart Association.Circulation. 2025 Feb 25;151(8):e41-e660. doi: 10.1161/CIR.0000000000001303. Epub 2025 Jan 27. Circulation. 2025. PMID: 39866113 Review.
-
Association between body shape index and coronary heart disease in individuals over 20 years old with obese.J Health Popul Nutr. 2024 Aug 16;43(1):123. doi: 10.1186/s41043-024-00614-3. J Health Popul Nutr. 2024. PMID: 39152519 Free PMC article.
References
-
- Cubanski J, Neuman T, White C. The Latest on Geographic Variation in Medicare Spending: A Demographic Divide Persists But Variation Has Narrowed. The Kaiser Family Foundation. 2015 http://kff.org/medicare/report/the-latest-on-geographic-variation-in-med.... Accessed September 28th, 2017.
-
- Newhouse JP, Garber AM. Geographic variation in health care spending in the United States: insights from an Institute of Medicine report. JAMA. 2013;310:1227–1228. - PubMed
-
- Centers for Medicare and Medicaid Services. Hospital Value-Based Purchasing: The Official Website for the Medicare Hospital Value-based Purchasing Program. 2014 http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instr.... Accessed June 4, 2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
