

Exercise Therapy and Cardiovascular Toxicity in Cancer
- PMID: 29530893
- PMCID: PMC6028047
- DOI: 10.1161/CIRCULATIONAHA.117.024671
Exercise Therapy and Cardiovascular Toxicity in Cancer
Abstract
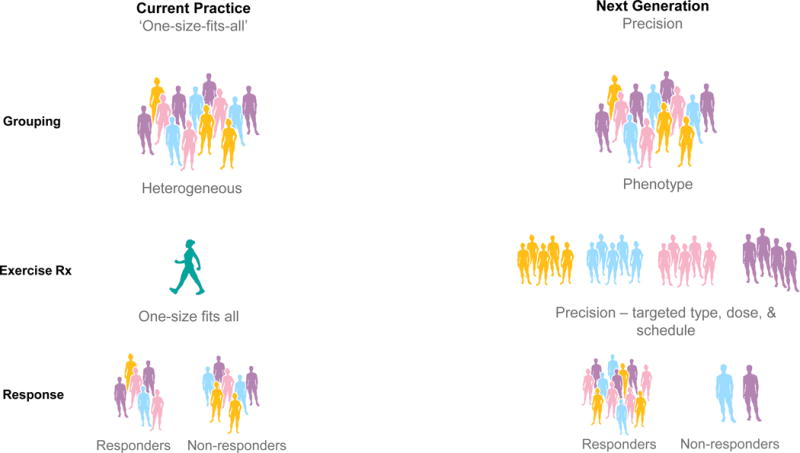
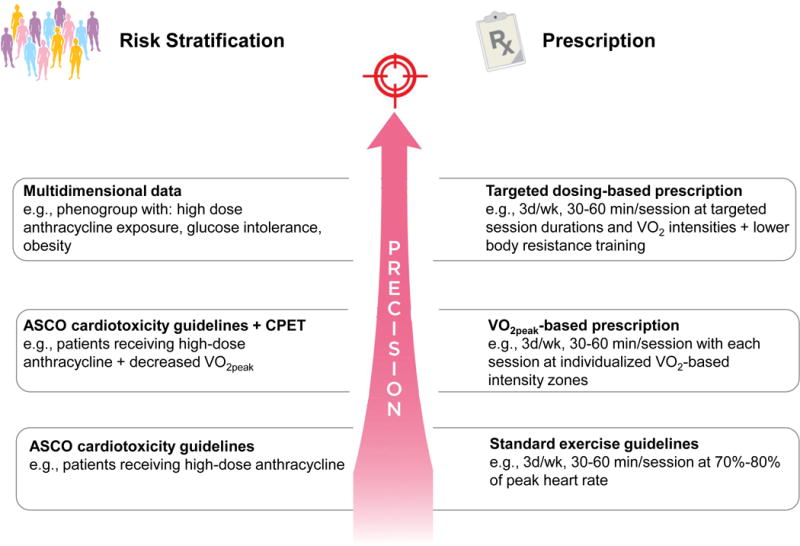
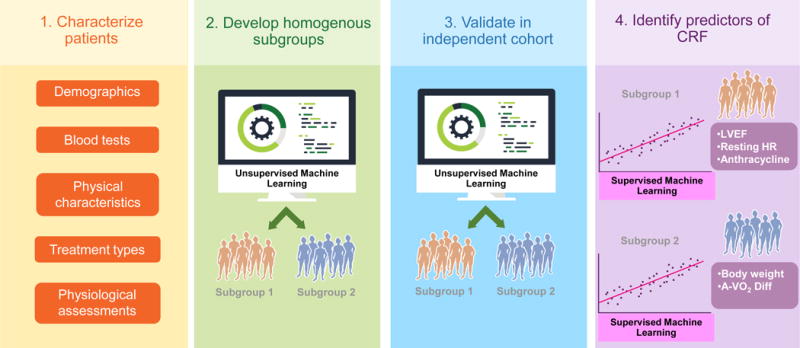
Cardio-oncology is an emerging discipline focused predominantly on the detection and management of cancer treatment-induced cardiac dysfunction (cardiotoxicity), which predisposes to development of overt heart failure or coronary artery disease. The direct adverse consequences, as well as those secondary to anticancer therapeutics, extend beyond the heart, however, to affect the entire cardiovascular-skeletal muscle axis (ie, whole-organism cardiovascular toxicity). The global nature of impairment creates a strong rationale for treatment strategies that augment or preserve global cardiovascular reserve capacity. In noncancer clinical populations, exercise training is an established therapy to improve cardiovascular reserve capacity, leading to concomitant reductions in cardiovascular morbidity and its attendant symptoms. Here, we overview the tolerability and efficacy of exercise on cardiovascular toxicity in adult patients with cancer. We also propose a conceptual research framework to facilitate personalized risk assessment and the development of targeted exercise prescriptions to optimally prevent or manage cardiovascular toxicity after a cancer diagnosis.
Keywords: cardiorespiratory fitness; cardiotoxicity; exercise; heart failure; survivorship.
© 2018 American Heart Association, Inc.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Perry S. Reduction of toxicity in cancer chemotherapy. Cancer Res. 1969;29:2319–2325. - PubMed
-
- Chabner BA, Roberts TG., Jr Timeline: Chemotherapy and the war on cancer. Nat Rev Cancer. 2005;5:65–72. - PubMed
-
- Bristow MR, Mason JW, Billingham ME, Daniels JR. Doxorubicin cardiomyopathy: evaluation by phonocardiography, endomyocardial biopsy, and cardiac catheterization. Ann Intern Med. 1978;88:168–175. - PubMed
-
- Lefrak EA, Pitha J, Rosenheim S, Gottlieb JA. A clinicopathologic analysis of adriamycin cardiotoxicity. Cancer. 1973;32:302–314. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
