

Predicting cancer outcomes from histology and genomics using convolutional networks
- PMID: 29531073
- PMCID: PMC5879673
- DOI: 10.1073/pnas.1717139115
Predicting cancer outcomes from histology and genomics using convolutional networks
Abstract
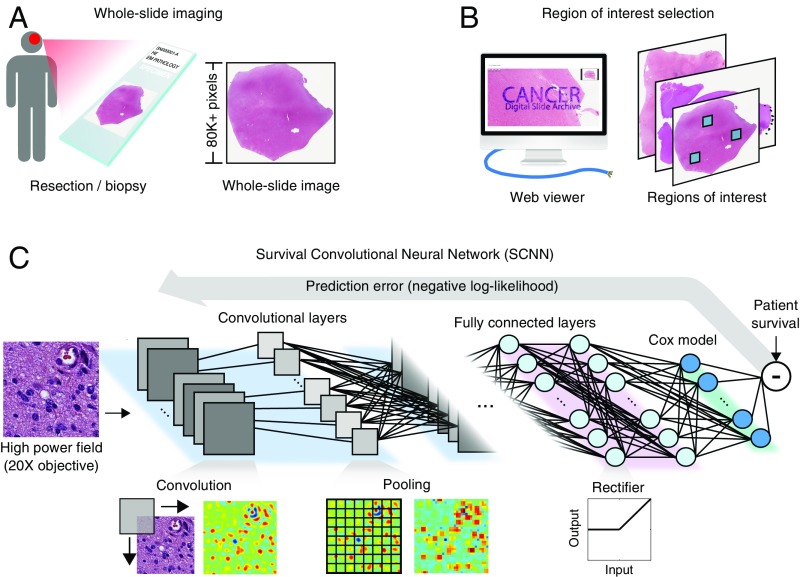
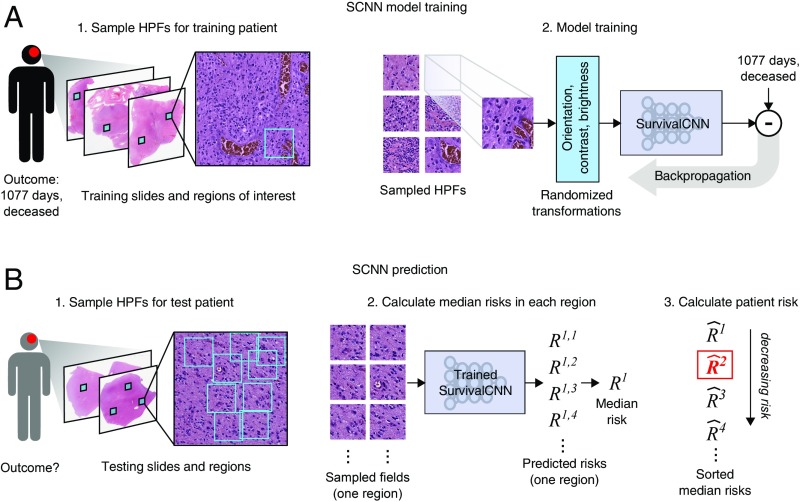
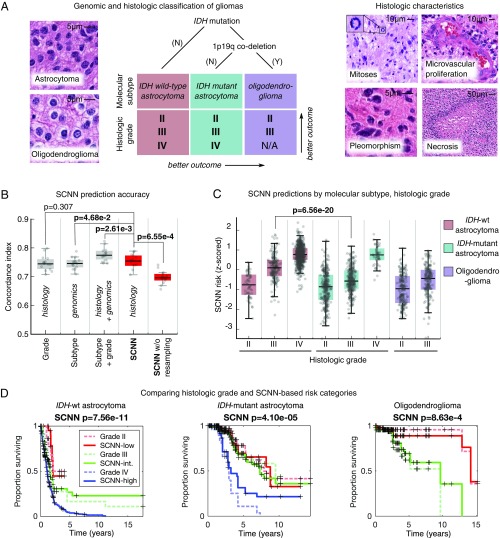
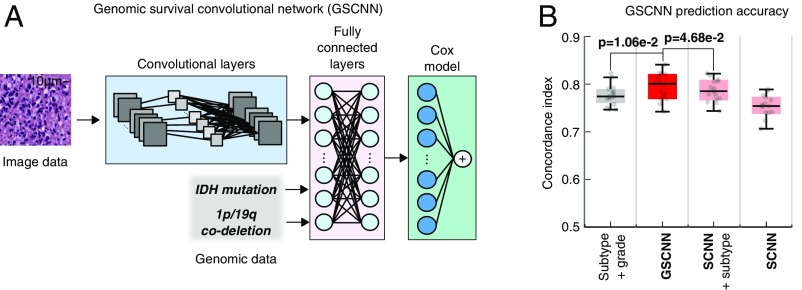
Cancer histology reflects underlying molecular processes and disease progression and contains rich phenotypic information that is predictive of patient outcomes. In this study, we show a computational approach for learning patient outcomes from digital pathology images using deep learning to combine the power of adaptive machine learning algorithms with traditional survival models. We illustrate how these survival convolutional neural networks (SCNNs) can integrate information from both histology images and genomic biomarkers into a single unified framework to predict time-to-event outcomes and show prediction accuracy that surpasses the current clinical paradigm for predicting the overall survival of patients diagnosed with glioma. We use statistical sampling techniques to address challenges in learning survival from histology images, including tumor heterogeneity and the need for large training cohorts. We also provide insights into the prediction mechanisms of SCNNs, using heat map visualization to show that SCNNs recognize important structures, like microvascular proliferation, that are related to prognosis and that are used by pathologists in grading. These results highlight the emerging role of deep learning in precision medicine and suggest an expanding utility for computational analysis of histology in the future practice of pathology.
Keywords: artificial intelligence; cancer; deep learning; digital pathology; machine learning.
Copyright © 2018 the Author(s). Published by PNAS.
Conflict of interest statement
Conflict of interest statement: L.A.D.C. leads a research project that is financially supported by Ventana Medical Systems, Inc. While this project is not directly related to the manuscript, it is in the general area of digital pathology.
Figures
References
-
- Kong J, et al. Computer-assisted grading of neuroblastic differentiation. Arch Pathol Lab Med. 2008;132:903–904, author reply 904. - PubMed
-
- Niazi MKK, et al. Visually meaningful histopathological features for automatic grading of prostate cancer. IEEE J Biomed Health Inform. 2017;21:1027–1038. - PubMed
-
- Naik S, et al. Proceedings of the 2008 5th IEEE International Symposium on Biomedical Imaging: From Nano to Macro. IEEE; Piscataway, NJ: 2008. Automated gland and nuclei segmentation for grading of prostate and breast cancer histopathology; pp. 284–287.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
