

Salivary cortisol in the diagnosis of adrenal insufficiency: cost efficient and patient friendly
- PMID: 29531158
- PMCID: PMC5890080
- DOI: 10.1530/EC-18-0085
Salivary cortisol in the diagnosis of adrenal insufficiency: cost efficient and patient friendly
Abstract
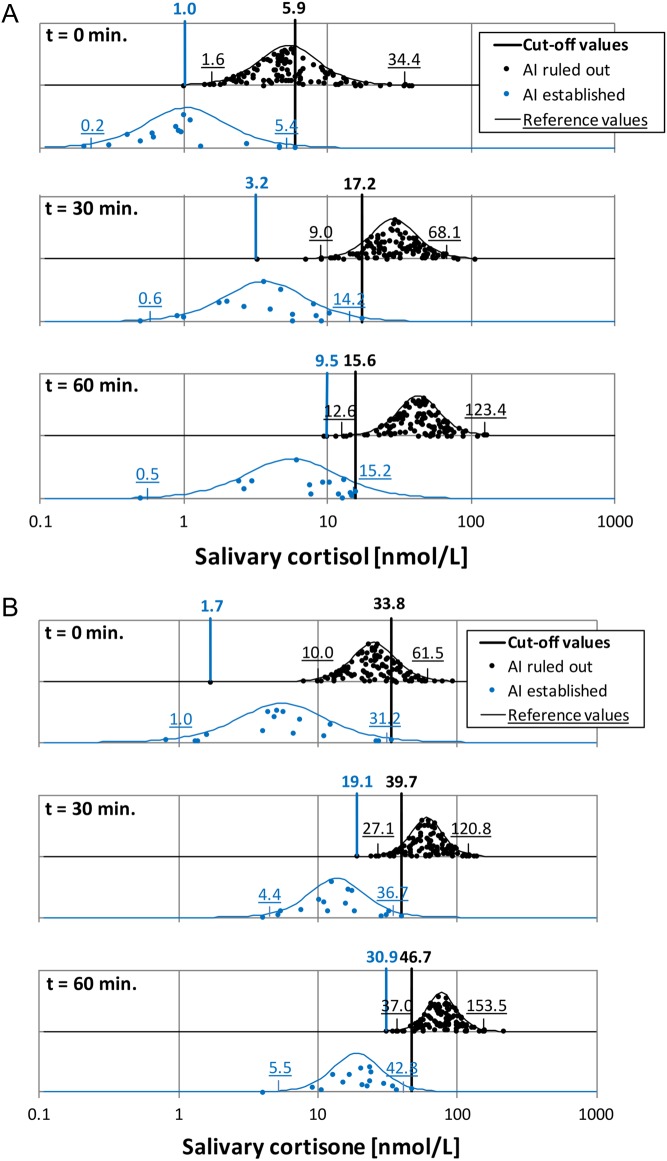
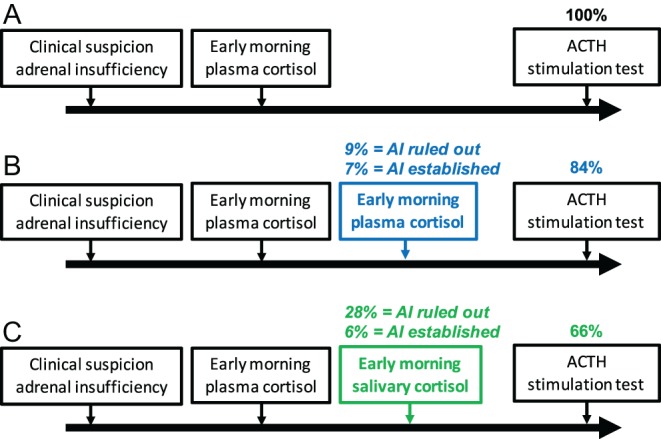
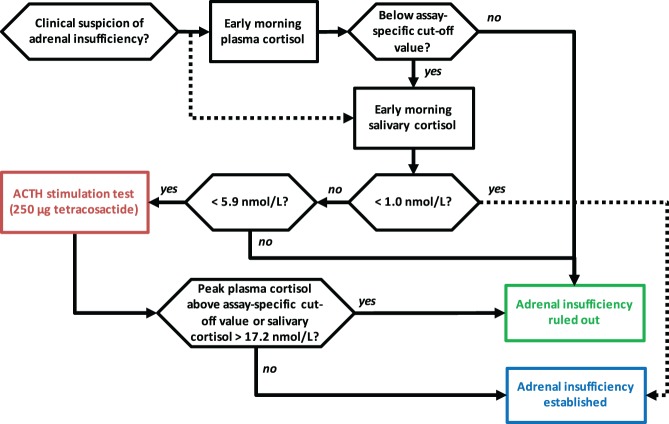
Saliva as a diagnostic tool is patient friendly and offers analytical advantages. Hormonal analysis of saliva is not influenced by changes in concentrations of binding globulins as the free concentration of the hormones is measured. Analysis of salivary cortisol is common practice in the diagnostic work-up of hypercortisolism. We investigated the potential role of measuring salivary cortisol when adrenal insufficiency (AI) is suspected, to reduce the numbers of ACTH stimulation tests. Over a period of 6 years, patients undergoing an ACTH stimulation test (tetracosactide, 250 µg) in our hospital were included. Plasma cortisol (Elecsys, Cobas, Roche Diagnostics) and salivary cortisol and cortisone (LC-MS/MS) were determined at t = 0, 30 and 60 min after stimulation. Based on peak plasma cortisol levels, AI was ruled out in 113 patients and was established in 16 patients. Patients without AI displayed maximal salivary cortisol concentrations of 12.6-123.4 nmol/L (95th percentile) after stimulation, as opposed to 0.5-15.2 nmol/L in AI patients. At t = 0 min, a minimal salivary cortisol concentration of 1.0 nmol/L was observed in patients without AI, whereas AI patients had a maximum concentration of 5.9 nmol/L. Using these cut-off values, 34% of the initial patient group could be diagnosed without an ACTH stimulation test (28% >5.9 nmol/L, 6% <1.0 nmol/L). A novel diagnostic algorithm, including early morning salivary cortisol analysis can reduce the numbers of ACTH stimulation tests in patients suspected of AI. This patient-friendly method can thereby reduce total health care costs.
Keywords: LC–MS/MS; adrenal insufficiency; cut-off values; salivary cortisol.
© 2018 The authors.
Figures
References
-
- Bornstein SR, Allolio B, Arlt W, Barthel A, Don-Wauchope A, Hammer GD, Husebye ES, Merke DP, Murad MH, Stratakis CA, et al Diagnosis and treatment of primary adrenal insufficiency: an Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology and Metabolism 2016. 101 364–389. (10.1210/jc.2015-1710) - DOI - PMC - PubMed
-
- VigiBase. Uppsala, Sweden: Uppsala Monitoring Centre, 2016. (available at: http://www.who-umc.org/)
LinkOut - more resources
Full Text Sources
Other Literature Sources
