

Predicting 131I-avidity of metastases from differentiated thyroid cancer using 18F-FDG PET/CT in postoperative patients with elevated thyroglobulin
- PMID: 29531251
- PMCID: PMC5847528
- DOI: 10.1038/s41598-018-22656-4
Predicting 131I-avidity of metastases from differentiated thyroid cancer using 18F-FDG PET/CT in postoperative patients with elevated thyroglobulin
Abstract
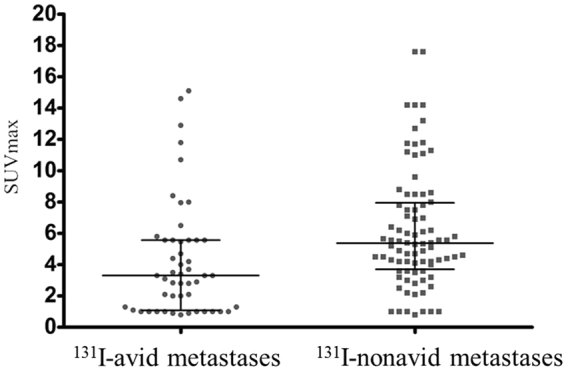
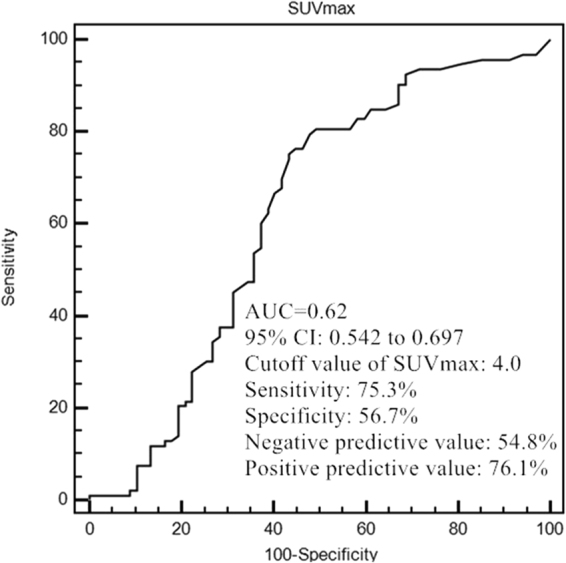
The quantitative relationship between iodine and glucose metabolism in metastases from differentiated thyroid cancer (DTC) remains unknown. Aim of the prospective study was to establish the value of 18F-FDG PET/CT in predicting 131I-avidity of metastases from DTC before the first radioiodine therapy. A total of 121 postoperative DTC patients with elevated stimulated serum thyroglobulin (ssTg) who underwent 131I adjuvant therapy or therapy after 18F-FDG PET/CT scan were enrolled. The Receiver operating characteristic curve was established to create an optimal cut-off point and evaluate the value of SUVmax for predicting 131I-avidity. In our study, the median SUVmax in 131I-nonavid metastatic target lesions was also significantly higher than that in 131I-avid metastatic target lesions (5.37 vs. 3.30; P = 0.000). At a cut-off value of 4.0 in SUVmax, the area under curve was 0.62 with the sensitivity, specificity, positive predictive value and negative predictive value of 75.3%, 56.7%, 76.1%, and 54.8%, respectively. These results suggest that 18F-FDG PET/CT may be of great value in identifying metastases in postoperative DTC patients with elevated ssTg before 131I administration, leading to an improved management of disease. 18F-FDG positive metastatic DTC with SUVmax of greater than 4.0 possesses higher probability of non-avidity to radioiodine.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Haugen BR, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26:1–133. doi: 10.1089/thy.2015.0020. - DOI - PMC - PubMed
-
- Cheng L, Liu M, Ruan M, Chen L. Challenges and strategies on radioiodine treatment for differentiated thyroid carcinoma. Hell. J. Nucl Med. 2016;19:23–32. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
