

Effect of a Digital Health Intervention on Receipt of Colorectal Cancer Screening in Vulnerable Patients: A Randomized Controlled Trial
- PMID: 29532054
- PMCID: PMC6033519
- DOI: 10.7326/M17-2315
Effect of a Digital Health Intervention on Receipt of Colorectal Cancer Screening in Vulnerable Patients: A Randomized Controlled Trial
Abstract
Background: Screening for colorectal cancer (CRC) reduces mortality, yet more than one third of age-eligible Americans are unscreened.
Objective: To examine the effect of a digital health intervention, Mobile Patient Technology for Health-CRC (mPATH-CRC), on rates of CRC screening.
Design: Randomized clinical trial. (ClinicalTrials.gov: NCT02088333).
Setting: 6 community-based primary care practices.
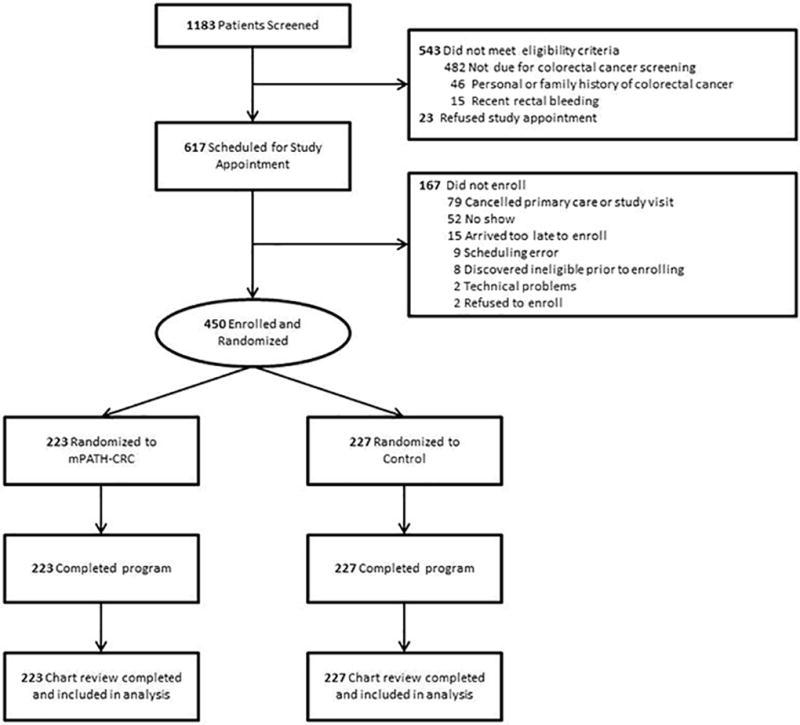
Participants: 450 patients (223 in the mPATH-CRC group and 227 in usual care) scheduled for a primary care visit and due for routine CRC screening.
Intervention: An iPad application that displays a CRC screening decision aid, lets patients order their own screening tests, and sends automated follow-up electronic messages to support patients.
Measurements: The primary outcome was chart-verified completion of CRC screening within 24 weeks. Secondary outcomes were ability to state a screening preference, intention to receive screening, screening discussions, and orders for screening tests. All outcome assessors were blinded to randomization.
Results: Baseline characteristics were similar between groups; 37% of participants had limited health literacy, and 53% had annual incomes less than $20 000. Screening was completed by 30% of mPATH-CRC participants and 15% of those receiving usual care (logistic regression odds ratio, 2.5 [95% CI, 1.6 to 4.0]). Compared with usual care, more mPATH-CRC participants could state a screening preference, planned to be screened within 6 months, discussed screening with their provider, and had a screening test ordered. Half of mPATH-CRC participants (53%; 118 of 223) "self-ordered" a test via the program.
Limitation: Participants were English speakers in a single health care system.
Conclusion: A digital health intervention that allows patients to self-order tests can increase CRC screening. Future research should identify methods for implementing similar interventions in clinical care.
Primary funding source: National Cancer Institute.
Comment in
-
Does Using an iPad Make an Intervention Innovative?Ann Intern Med. 2018 Apr 17;168(8):592-593. doi: 10.7326/M18-0346. Epub 2018 Mar 13. Ann Intern Med. 2018. PMID: 29532079 No abstract available.
References
-
- Inadomi JM. Screening for Colorectal Neoplasia. N Engl J Med. 2017 Jan 12;376(2):149–56. - PubMed
-
- Ladabaum U, Mannalithara A. Comparative Effectiveness and Cost Effectiveness of a Multitarget Stool DNA Test to Screen for Colorectal Neoplasia. Gastroenterology. 2016 Sep;151(3):427–439.e6. - PubMed
-
- Lin JS, Piper MA, Perdue LA, Rutter C, Webber EM, O’Connor E, et al. Screening for Colorectal Cancer: A Systematic Review for the U.S. Preventive Services Task Force. Rockville (MD): Agency for Healthcare Research and Quality (US); 2016. Report No: 14-05203-EF-1. - PubMed
-
- Patel SS, Kilgore ML. Cost Effectiveness of Colorectal Cancer Screening Strategies. Cancer Control J Moffitt Cancer Cent. 2015 Apr;22(2):248–58. - PubMed
-
- Sharaf RN, Ladabaum U. Comparative Effectiveness and Cost-Effectiveness of Screening Colonoscopy vs. Sigmoidoscopy and Alternative Strategies. Am J Gastroenterol. 2013 Jan;108(1):120–32. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical