

Association of Hospital Performance Based on 30-Day Risk-Standardized Mortality Rate With Long-term Survival After Heart Failure Hospitalization: An Analysis of the Get With The Guidelines-Heart Failure Registry
- PMID: 29532056
- PMCID: PMC5875302
- DOI: 10.1001/jamacardio.2018.0579
Association of Hospital Performance Based on 30-Day Risk-Standardized Mortality Rate With Long-term Survival After Heart Failure Hospitalization: An Analysis of the Get With The Guidelines-Heart Failure Registry
Abstract
Importance: Among patients hospitalized with heart failure (HF), the long-term clinical implications of hospitalization at hospitals based on 30-day risk-standardized mortality rates (RSMRs) is not known.
Objective: To evaluate the association of hospital-specific 30-day RSMR with long-term survival among patients hospitalized with HF in the American Heart Association Get With The Guidelines-HF registry.
Design, setting, and participants: The longitudinal observational study included 106 304 patients with HF who were admitted to 317 centers participating in the Get With The Guidelines-HF registry from January 1, 2005, to December 31, 2013, and had Medicare-linked follow-up data. Hospital-specific 30-day RSMR was calculated using a hierarchical logistic regression model. In the model, 30-day mortality rate was a binary outcome, patient baseline characteristics were included as covariates, and the hospitals were treated as random effects. The association of 30-day RSMR-based hospital groups (low to high 30-day RSMR: quartile 1 [Q1] to Q4) with long-term (1-year, 3-year, and 5-year) mortality was assessed using adjusted Cox models. Data analysis took place from June 29, 2017, to February 19, 2018.
Exposures: Thirty-day RSMR for participating hospitals.
Main outcomes and measures: One-year, 3-year, and 5-year mortality rates.
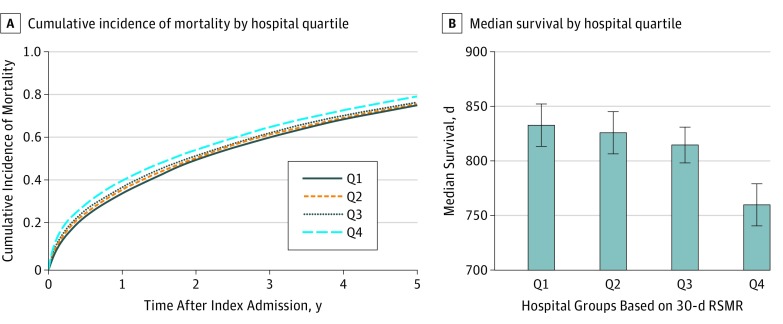
Results: Of the 106 304 patients included in the analysis, 57 552 (54.1%) were women and 84 595 (79.6%) were white, and the median (interquartile range) age was 81 (74-87) years. The 30-day RSMR ranged from 8.6% (Q1) to 10.7% (Q4). Hospitals in the low 30-day RSMR group had greater availability of advanced HF therapies, cardiac surgery, and percutaneous coronary interventions. In the primary landmarked analyses among 30-day survivors, there was a graded inverse association between 30-day RSMR and long-term mortality (Q1 vs Q4: 5-year mortality, 73.7% vs 76.8%). In adjusted analysis, patients admitted to hospitals in the high 30-day RSMR group had 14% (95% CI, 10-18) higher relative hazards of 5-year mortality compared with those admitted to hospitals in the low 30-day RSMR group. Similar findings were observed in analyses of survival from admission, with 22% (95% CI, 18-26) higher relative hazards of 5-year mortality for patients admitted to Q4 vs Q1 hospitals.
Conclusions and relevance: Lower hospital-level 30-day RSMR is associated with greater 1-year, 3-year, and 5-year survival for patients with HF. These differences in 30-day survival continued to accrue beyond 30 days and persisted long term, suggesting that 30-day RSMR may be a useful HF performance metric to incentivize quality care and improve long-term outcomes.
Conflict of interest statement
Figures
Similar articles
-
Evaluation of Risk-Adjusted Home Time After Hospitalization for Heart Failure as a Potential Hospital Performance Metric.JAMA Cardiol. 2021 Feb 1;6(2):169-176. doi: 10.1001/jamacardio.2020.4928. JAMA Cardiol. 2021. PMID: 33112393 Free PMC article.
-
Association Between Hospital Volume, Processes of Care, and Outcomes in Patients Admitted With Heart Failure: Insights From Get With The Guidelines-Heart Failure.Circulation. 2018 Apr 17;137(16):1661-1670. doi: 10.1161/CIRCULATIONAHA.117.028077. Epub 2018 Jan 29. Circulation. 2018. PMID: 29378692
-
Association of readmission penalty amount with subsequent 30-day risk standardized readmission and mortality rates among patients hospitalized with heart failure: An analysis of get with the guidelines - heart failure participating centers.Am Heart J. 2022 Apr;246:1-11. doi: 10.1016/j.ahj.2021.12.014. Epub 2021 Dec 30. Am Heart J. 2022. PMID: 34973189
-
Association of pre-hospital precipitating factors with short- and long-term outcomes of acute heart failure patients: A report from the WET-HF2 registry.Int J Cardiol. 2023 Oct 15;389:131161. doi: 10.1016/j.ijcard.2023.131161. Epub 2023 Jul 10. Int J Cardiol. 2023. PMID: 37437664 Review.
-
Sex-specific differences drive temporal trends and outcomes of patients hospitalized for heart failure in Germany.Prog Cardiovasc Dis. 2020 Sep-Oct;63(5):591-598. doi: 10.1016/j.pcad.2020.03.013. Epub 2020 Mar 26. Prog Cardiovasc Dis. 2020. PMID: 32224115 Review.
Cited by
-
Population-Level Implications of Sodium-Glucose Cotransporter-2 Inhibitors for Heart Failure With Preserved Ejection Fraction in the US.JAMA Cardiol. 2023 Jan 1;8(1):66-73. doi: 10.1001/jamacardio.2022.4348. JAMA Cardiol. 2023. PMID: 36334258 Free PMC article.
-
Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association.Circulation. 2023 Feb 21;147(8):e93-e621. doi: 10.1161/CIR.0000000000001123. Epub 2023 Jan 25. Circulation. 2023. PMID: 36695182 Free PMC article. Review.
-
Unplanned 30-day readmissions, comorbidity and impact on one-year mortality following incident heart failure hospitalisation in Western Australia, 2001-2015.BMC Cardiovasc Disord. 2023 Jan 16;23(1):25. doi: 10.1186/s12872-022-03020-x. BMC Cardiovasc Disord. 2023. PMID: 36647020 Free PMC article.
-
Effectiveness of Telemedicine Visits in Reducing 30-Day Readmissions Among Patients With Heart Failure During the COVID-19 Pandemic.J Am Heart Assoc. 2022 Apr 5;11(7):e023935. doi: 10.1161/JAHA.121.023935. Epub 2022 Mar 1. J Am Heart Assoc. 2022. PMID: 35229656 Free PMC article.
-
Sequential organ failure assessment score on admission predicts long-term mortality in acute heart failure patients.ESC Heart Fail. 2020 Feb;7(1):244-252. doi: 10.1002/ehf2.12563. Epub 2020 Jan 6. ESC Heart Fail. 2020. PMID: 31905270 Free PMC article.
References
-
- Mozaffarian D, Benjamin EJ, Go AS, et al. ; Writing Group Members; American Heart Association Statistics Committee; Stroke Statistics Subcommittee . Executive summary: heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation. 2016;133(4):447-454. - PubMed
-
- US Centers for Medicare and Medicaid Services Hospital quality initiative: outcome measures. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Inst.... Accessed November 18, 2017.
-
- Medicare Program; hospital inpatient prospective payment systems for acute care hospitals and the long-term care hospital prospective payment system and fiscal year 2014 rates; quality reporting requirements for specific providers; hospital conditions of participation; payment policies related to patient status. Fed Regist. 2013;78(160):50676-50729. - PubMed
-
- Medicare Program; hospital inpatient prospective payment systems for acute care hospitals and the long-term care hospital prospective payment system and fiscal year 2014 rates; quality reporting requirements for specific providers; hospital conditions of participation; payment policies related to patient status. Fed Regist. 2013;78(160):50649-50676. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
