

Closing the Referral Loop: an Analysis of Primary Care Referrals to Specialists in a Large Health System
- PMID: 29532299
- PMCID: PMC5910374
- DOI: 10.1007/s11606-018-4392-z
Closing the Referral Loop: an Analysis of Primary Care Referrals to Specialists in a Large Health System
Abstract
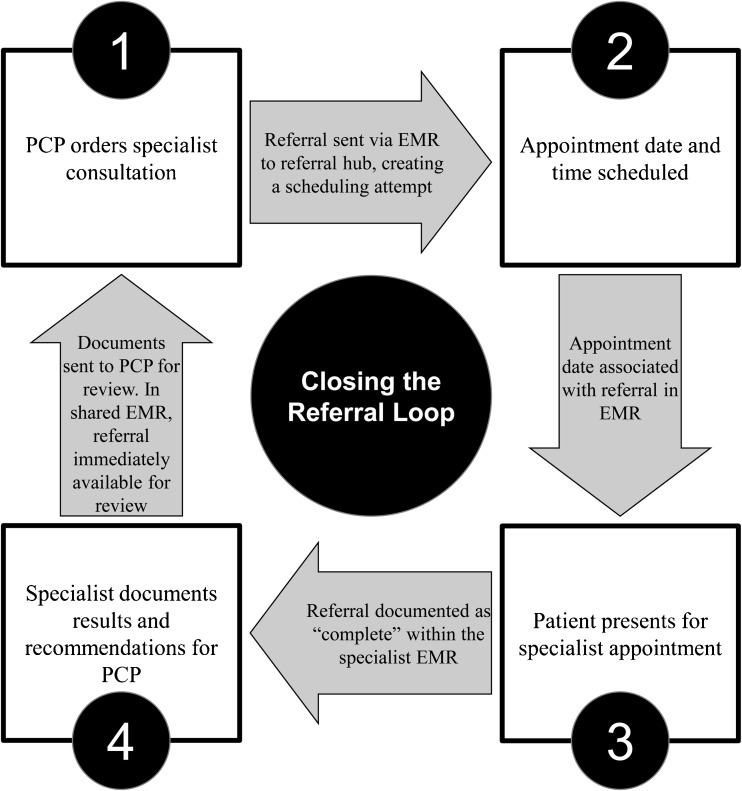
Purpose: Ideally, a referral from a primary care physician (PCP) to a specialist results in a completed specialty appointment with results available to the PCP. This is defined as "closing the referral loop." As health systems grow more complex, regulatory bodies increase vigilance, and reimbursement shifts towards value, closing the referral loop becomes a patient safety, regulatory, and financial imperative.
Objective/design: To assess the ability of a large health system to close the referral loop, we used electronic medical record (EMR)-generated data to analyze referrals from a large primary care network to 20 high-volume specialties between July 1, 2015 and June 30, 2016.
Main measures: The primary metric was documented specialist appointment completion rate. Explanatory analyses included documented appointment scheduling rate, individual clinic differences, appointment wait times, and geographic distance to appointments.
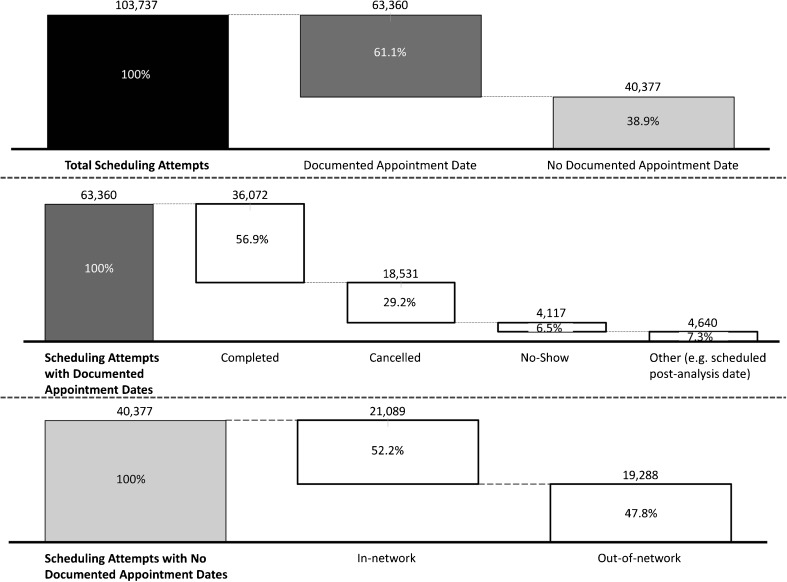
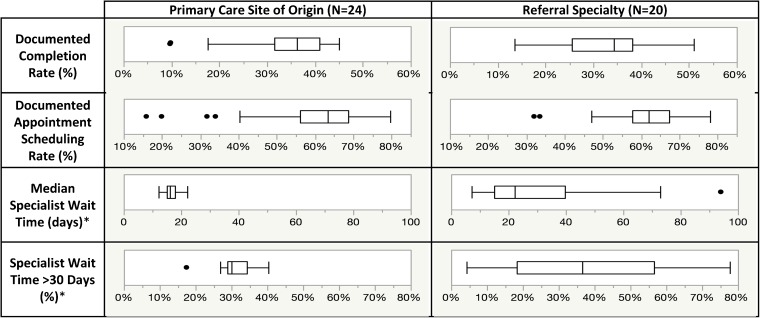
Key results: Of the 103,737 analyzed referral scheduling attempts, only 36,072 (34.8%) resulted in documented complete appointments. Low documented appointment scheduling rates (38.9% of scheduling attempts lacked appointment dates), individual clinic differences in closing the referral loop, and significant differences in wait times and distances to specialists between complete and incomplete appointments drove this gap. Other notable findings include high variation in wait times among specialties and correlation between high wait times and low documented appointment completion rates.
Conclusions: The rate of closing the referral loop in this health system is low. Low appointment scheduling rates, individual clinic differences, and patient access issues of wait times and geographic proximity explain much of the gap. This problem is likely common among large health systems with complex provider networks and referral scheduling. Strategies that improve scheduling, decrease variation among clinics, and improve patient access will likely improve rates of closing the referral loop. More research is necessary to determine the impact of these changes and other potential driving factors.
Keywords: access to care; managed care; patient safety; population health; primary care redesign.
Conflict of interest statement
Dr. Bosworth receives research funds through Duke University from NIH, VA, Pharma foundation, Johnson & Johnson, Improved Patient Outcomes, Takeda, and Sanofi. He has received honorarium from Sanofi, Otsuka pharmaceuticals, Genentech, and has been a member of Boehringer Ingelheim Speaking bureau. Other authors report no conflicts of interest.
Figures
References
-
- Additional Information Regarding EH Clinical Quality Measures. In: Services CfMM, ed. Baltimore, MD: United States Federal Government; 2014.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
