

Pooled Analyses of Phase III Studies of ADS-5102 (Amantadine) Extended-Release Capsules for Dyskinesia in Parkinson's Disease
- PMID: 29532440
- PMCID: PMC5934466
- DOI: 10.1007/s40263-018-0498-4
Pooled Analyses of Phase III Studies of ADS-5102 (Amantadine) Extended-Release Capsules for Dyskinesia in Parkinson's Disease
Erratum in
-
Author Correction to: Pooled Analyses of Phase III Studies of ADS-5102 (Amantadine) Extended-Release Capsules for Dyskinesia in Parkinson's Disease.CNS Drugs. 2018 Apr;32(4):399-400. doi: 10.1007/s40263-018-0510-z. CNS Drugs. 2018. PMID: 29637528 Free PMC article.
Abstract
Background: Although levodopa is considered the most effective pharmacotherapy for motor symptoms of Parkinson's disease (PD), chronic use is associated with motor complications, including fluctuating response and unpredictable, involuntary movements called dyskinesia. ADS-5102 (amantadine) extended-release (ER) capsules (GOCOVRITM) is a recent US FDA-approved treatment for dyskinesia in PD patients. ADS-5102 is a high-dose, ER formulation of amantadine, administered orally once daily at bedtime, that achieves high plasma drug concentrations throughout the day.
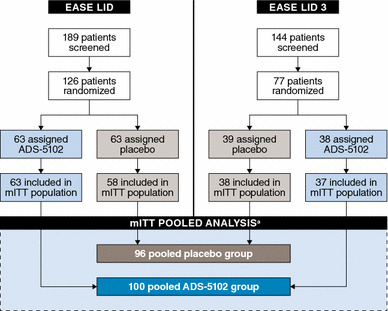
Objective: In this study, we present pooled results from two randomized, double-blind, placebo-controlled, phase III ADS-5102 trials.
Patients and methods: The two studies in PD patients with dyskinesia shared design and eligibility criteria, differing only in treatment duration. Results from common assessment time points were pooled.
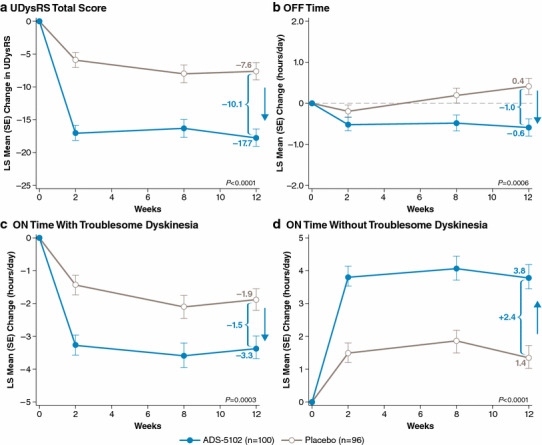
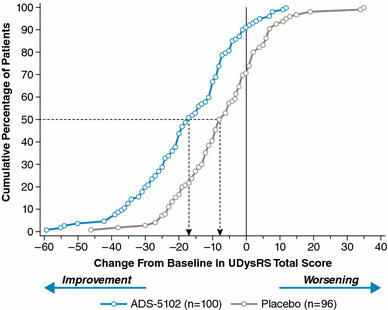
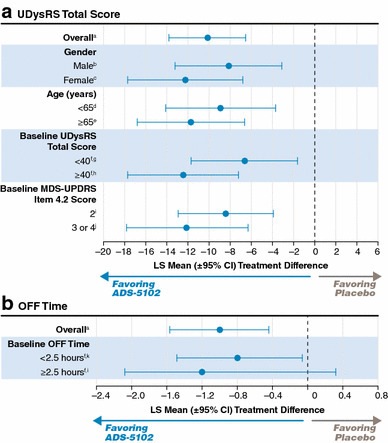
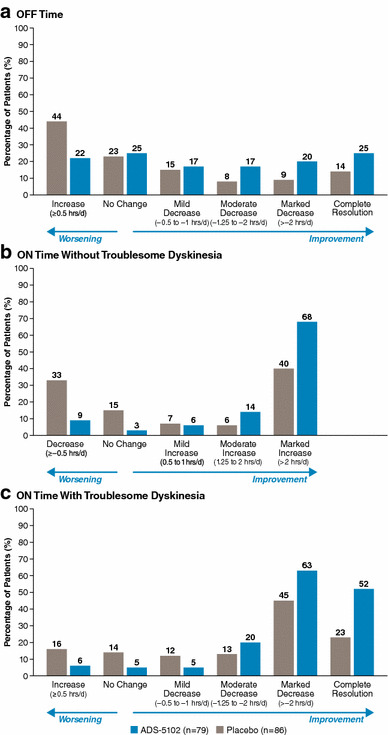
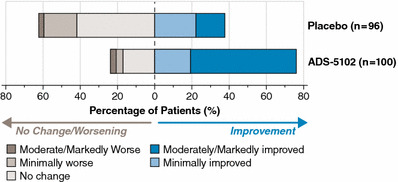
Results: At 12 weeks, the least squares (LS) mean change in total score on the Unified Dyskinesia Rating Scale among 100 patients randomized to ADS-5102 and 96 patients randomized to placebo was - 17.7 (standard error [SE] 1.3) vs. - 7.6 (1.3) points, respectively (- 10.1 points, 95% confidence interval [CI] - 13.8, - 6.5; p < 0.0001). The relative treatment difference between groups was 27.3% (p < 0.0001). At 12 weeks, the LS mean change in OFF time was - 0.59 (0.21) vs. +0.41 (0.20) h/day, a difference of - 1.00 h/day (95% CI - 1.57, - 0.44; p = 0.0006). For both efficacy measures, a significant difference from placebo was attained by two weeks, the first post-baseline assessment, and was maintained throughout 12 weeks. In the pooled ADS-5102 group, the most common adverse events were hallucination, dizziness, dry mouth, peripheral edema, constipation, falls, and orthostatic hypotension.
Conclusions: These analyses provide further evidence supporting ADS-5102 as an adjunct to levodopa for treating both dyskinesia and OFF time in PD patients with dyskinesia. Clinicaltrials.gov identifier: NCT02136914 and NCT02274766.
Conflict of interest statement
Lawrence W. Elmer has received honoraria for speaking engagements from Lundbeck, Novartis, UCB Pharma, and Teva Neuroscience; has served as a paid consultant for Teva Neuroscience and UCB Pharma; has received honoraria as a member of advisory boards for Lundbeck, Teva Neuroscience, and UCB Pharma; and has received unrestricted educational grant support from Teva Neuroscience. Jorge L. Juncos reports research grants from the National Institute of Child Health and Human Development (NICHD), the Michael J. Fox Foundation, Adamas Pharmaceuticals, US WorldMeds, Psydon, and Neurocrine. Carlos Singer has received honoraria from Neurocrine, Revance, US WorldMeds, TEVA, and Acorda, and has received grants from Allergan, Adams, Pfizer, Synovia, the Parkinson’s Foundation, National Institutes of Health (NIH), and the Huntington’s Disease Society of America. Daniel D. Truong has received research grants from Ispen, Merz, Auspex, Daiichi Sankyo Pharma, AbbVie, National Institute of Neurological Disorders and Stroke, Kyowa, and Neurocrine. Susan R. Criswell has no relevant disclosures or conflicts of interest. Sotirios Parashos has no relevant disclosures or conflicts of interest. Unrelated to the subject matter of this study, Sotirios Parashos has received consultancies from Dong-A, research support from the Park Nicollet Foundation, National Parkinson Foundation, NINDS, Patient-Centered Outcomes Research Institute, Acorda Therapeutics, Astellas, Pharma2B, and Sunovion Pharmaceuticals. Larissa Felt, Reed Johnson, and Rajiv Patni are employees of and own stock in Adamas Pharmaceuticals.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
