

Antimicrobial susceptibility trends and evolution of isolates with extended spectrum β-lactamases among Gram-negative organisms recovered during the SMART study in Spain (2011-2015)
- PMID: 29532655
- PMCID: PMC6159370
Antimicrobial susceptibility trends and evolution of isolates with extended spectrum β-lactamases among Gram-negative organisms recovered during the SMART study in Spain (2011-2015)
Abstract
Objective: The SMART (Study for Monitoring Antimicrobial Resistance Trends) surveillance study monitors antimicrobial susceptibility and extended spectrum β-lactamases (ESBLs) in Gram-negative bacilli recovered from intra-abdominal infections (IAI).
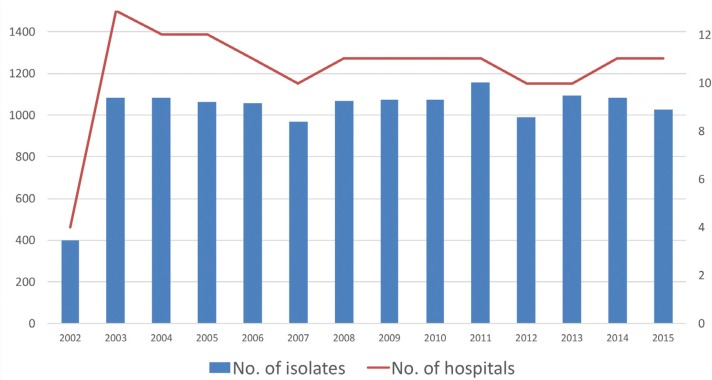
Methods: Antimicrobial susceptibility of 5,343 isolates from IAI recovered in 11 centres during the 2011-2015 SMART-Spain program was analysed by standard microdilution (EUCAST criteria) and compared with that from 2002-2010. ESBLs were phenotypically detected.
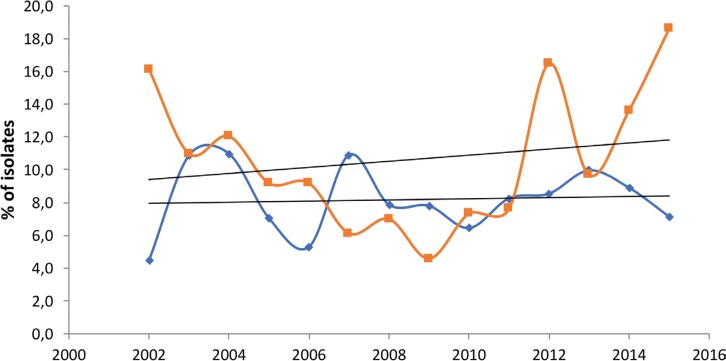
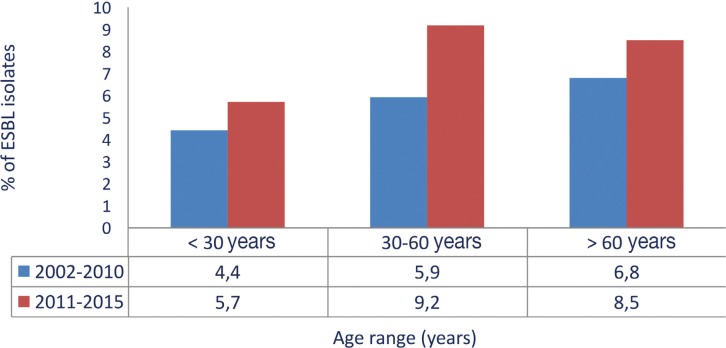
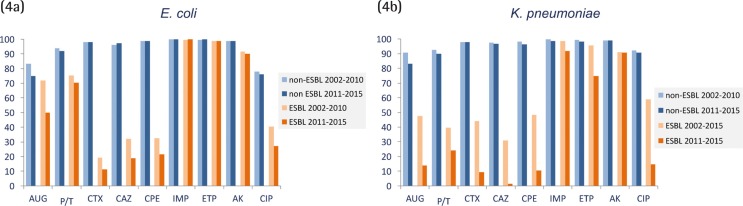
Results: Escherichia coli, the most common isolate, significantly decreased in community acquired IAI (60.9% 2002-2010 vs. 56.1% 2011-2015, P=0.0003). It was followed in prevalence by Klebsiella pneumoniae that increased both in the community (8.9% vs. 10.8%, P=0.016) and nosocomial (9.2% vs. 10.8%, P=0.029) IAI and P. aeruginosa, which significantly increased in community acquired IAI (5.6% vs. 8.0%, P=0.0003). ESBLs were more prevalent in K. pneumoniae (16.3%) than in E. coli (9.5%) of nosocomial origin and were more frequently isolated from elderly patients (>60 years). Considering all Enterobacteriaceae, ertapenem (92.3-100%) and amikacin (95.5%-100%) were the most active antimicrobials. Ertapenem activity, unlike amoxicillin-clavulanate or piperacillin-tazobactam, remained virtually unchanged in ESBL (100%) and non-ESBL (98.8%) E. coli producers. Its activity decreased in ESBL-K. pneumoniae (74.7%) but was higher than that of amoxicillin-clavulanate (14.0%) and piperacillin-tazobactam (24.0%). Interestingly, ertapenem susceptibility was maintained in >60% of ESBL isolates that were resistant to amoxicillin-clavulanate, piperacillin-tazobactam or fluoroquinolones.
Conclusions: SMART-Spain results support current guidelines which include ertapenem as empiric treatment in mild-moderate community-acquired IAI, particularly with ESBL producers. These recommendations will need to be updated with the recently introduction of new antimicrobials.
Introducción: El estudio SMART (Study for Monitoring Antimicrobial Resistance Trends) monitoriza la sensibilidad antimicrobiana y las β-lactamasas de espectro extendido (BLEE) en bacilos gramnegativos obtenidos de infecciones intraabdominales (IIA).
Material y Métodos: Se ha analizado la sensibilidad antimicrobiana (microdilución estándar, criterios EUCAST) y las BLEE (detección fenotípica) de 5.343 aislados de IIA en 11 centros del programa SMART-España durante 2011-2015 en comparación con 2002-2010.
Resultados: Escherichia coli, el microorganismo más prevalente, disminuyó significativamente en las IIA de origen comunitario (60,9% 2002-2010 vs. 56,1% 2011-2015, P=0,0003). Fue seguido en prevalencia por Klebsiella pneumoniae que aumentó tanto en IIA comunitaria (8,9% vs. 10,8%, P=0,016) como nosocomial (9,2% vs. 10,8%, P=0,029) y por P. aeruginosa que aumentó en la IIA comunitaria (5,6% vs. 8,0%, P=0,0003). Las BLEE fueron más prevalentes en la IIA nosocomial por K. pneumoniae (16,3%) que por E. coli (9,5%), siendo más frecuentes en pacientes de mayor edad (>60 años). Considerando todas las Enterobacteriaceae, ertapenem (92,3-100%) y amikacina (95,5%-100%) fueron los antimicrobianos más activos. La sensibilidad a ertapenem, al contrario que a amoxicilina-clavulánico o piperacilina-tazobactam, se mantuvo sin cambios en E. coli con (98,8%) y sin BLEE (100%). Su sensibilidad disminuyó en BLEE-K. pneumoniae (74,7%) pero fue mayor que la de amoxicilina-clavulánico (14,0%) o piperacilina-tazobactam (24,0%). Es de resaltar que esta actividad se mantuvo >60% en los aislados con BLEE resistentes a amoxicilina-clavulánico, piperacilina-tazobactam o fluoroquinolonas.
Conclusiones: El estudio SMART-España sustenta las guías actuales que incluyen al ertapenem como tratamiento empírico en la IIA leve-moderada comunitaria, en particular con BLEE. Estas recomendaciones precisaran actualizarse con la reciente introducción de nuevos antimicrobianos.
© The Author 2018. Published by Sociedad Española de Quimioterapia.
Conflict of interest statement
Rafael Cantón has collaborated in educational meetings sponsored by MSD, Pfizer and AstraZeneca. He has also had research grants from MSD and AstraZeneca. F. Javier Castillo has collaborated in educational meetings sponsored by MSD.
All other authors declare that they have no conflicts of interest regarding this publication.
Figures
References
-
- Sievert DM, Ricks P, Edwards JR, Schneider A, Patel J, Srinivasan A, et al. . Antimicrobial-resistant pathogens associated with healthcare-associated infections: summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2009–2010. Infect Control Hosp Epidemiol. 2013; 34:1–14. PMID: . - PubMed
-
- García-Sánchez JE, García-García MI, García-Garrote F, Sánchez-Romero I. Microbiological diagnosis of intra-abdominal infections. Enferm Infecc Microbiol Clin. 2013; 31:230-9PMID:. - PubMed
-
- Shirah GR, O’Neill PJ. Intra-abdominal infections. Surg Clin North Am. 2014; 94:1319-33. PMID: . - PubMed
-
- Skrupky LP, Tellor BR, Mazuski JE. Current strategies for the treatment of complicated intraabdominal infections. Expert Opin Pharmacother. 2013; 14:1933-47. PMID: . - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
