

Aflatoxin B1 exposure increases the risk of hepatocellular carcinoma associated with hepatitis C virus infection or alcohol consumption
- PMID: 29533866
- PMCID: PMC5895495
- DOI: 10.1016/j.ejca.2018.02.010
Aflatoxin B1 exposure increases the risk of hepatocellular carcinoma associated with hepatitis C virus infection or alcohol consumption
Abstract
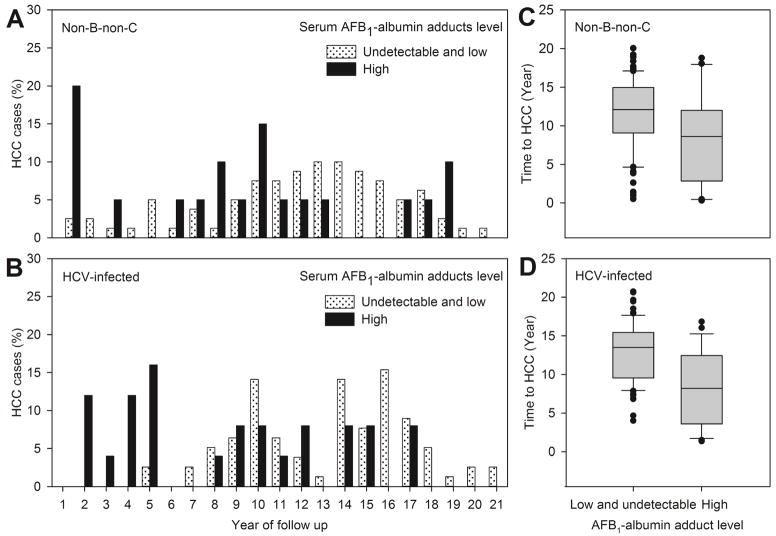
Background: Hepatocarcinogenicity of aflatoxin B1 (AFB1) has rarely been studied in populations with hepatitis C virus (HCV) infection and those without hepatitis B virus (HBV) and HCV infection (non-B-non-C). This case-control study nested in a community-based cohort aimed to investigate the HCC risk associated with AFB1 in HCV-infected and non-B-non-C participants.
Methods: Baseline serum AFB1-albumin adduct levels were measured in 100 HCC cases and 1767 controls seronegative for anti-HCV and HBsAg (non-B-non-C), and another 103 HCC cases and 176 controls who were anti-HCV-seropositive and HBsAg-seronegative. Odds ratios (ORs) and 95% confidence intervals (95% CIs) were estimated using logistic regression.
Results: In 20 years of follow-up, the follow-up time to newly developed HCC was significantly shorter in participants with higher serum AFB1-albumin adduct levels in non-B-non-C (p = 0.0162) and HCV-infected participants (p < 0.0001). Within 8 years of follow-up, HCV infection and AFB1 exposure were independent risk factors for HCC. Elevated serum AFB1-albumin adduct levels were significantly associated with an increased risk of HCC newly developed within 8 years of follow-up in non-B-non-C participants with habitual alcohol consumption [crude OR (95% CI) for high vs. low/undetectable levels, 4.22 (1.16-15.37)] and HCV-infected participants [3.39 (1.31-8.77)], but not in non-B-non-C participants without alcohol drinking habit. AFB1 exposure remained an independent risk predictor for HCV-related HCC after adjustment for other HCC predictors (multivariate-adjusted OR [95% CI], 3.65 [1.32-10.10]).
Conclusions: AFB1 exposure contributes to the development of HCC in participants with significant risk factors for cirrhosis including alcohol and HCV infection.
Keywords: Aflatoxin B(1); Albumin adducts; HCC; HCV infection; Habitual alcohol drinking.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
No potential conflicts of interest were disclosed.
Figures
References
-
- Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–86. - PubMed
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108. - PubMed
-
- Wild CP, Turner PC. The toxicology of aflatoxins as a basis for public health decisions. Mutagenesis. 2002;17:471–81. - PubMed
-
- Cullen JM, Newberne PM. Acute hepatotoxicity of aflatoxins. In: Eaton DL, Groopman JD, editors. The toxicology of aflatoxins: human health, veterinary, and agricultural significance. London: Academic Press; 1993. pp. 1–26.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
