

Any Place for Immunohistochemistry within the Predictive Biomarkers of Treatment in Lung Cancer Patients?
- PMID: 29534030
- PMCID: PMC5876645
- DOI: 10.3390/cancers10030070
Any Place for Immunohistochemistry within the Predictive Biomarkers of Treatment in Lung Cancer Patients?
Abstract
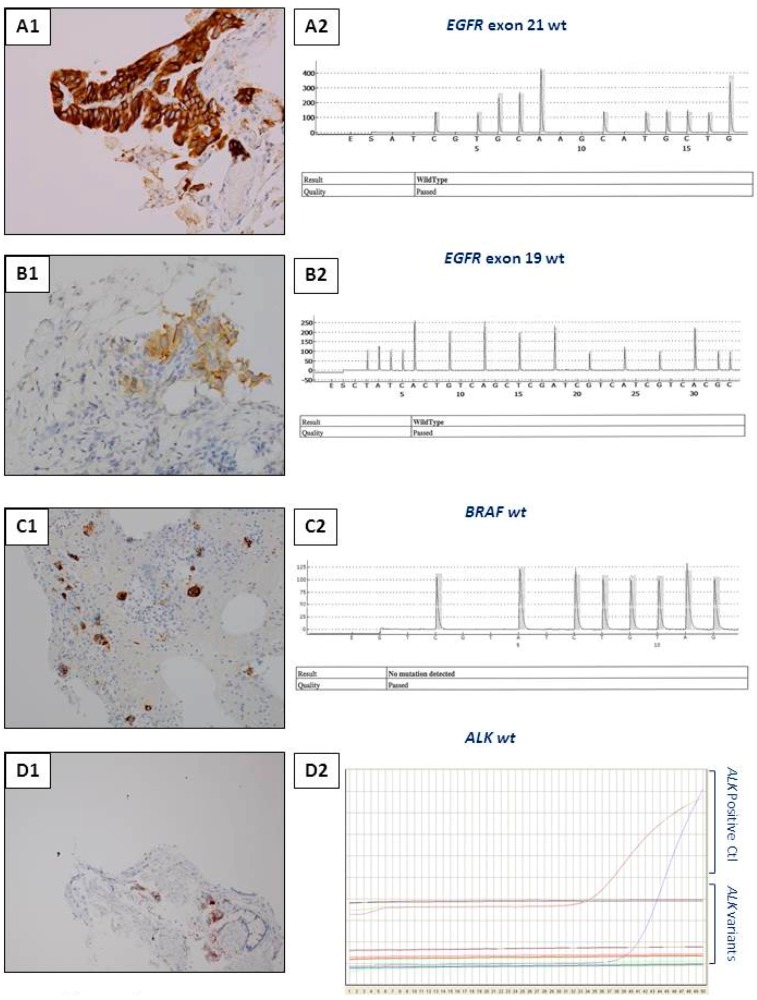
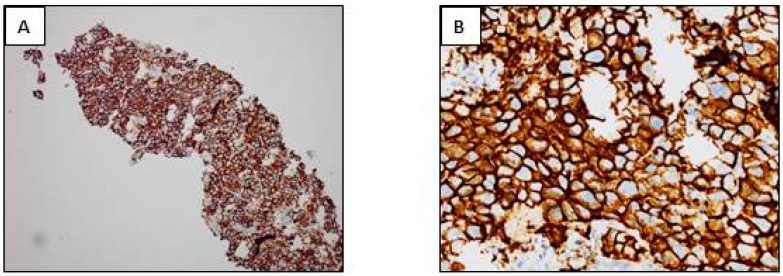
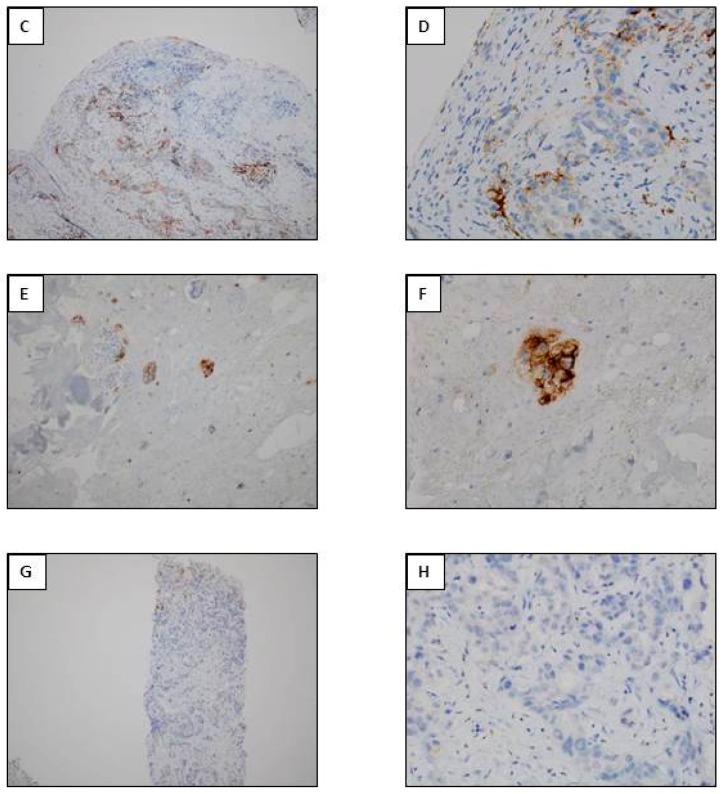
The identification of certain genomic alterations (EGFR, ALK, ROS1, BRAF) or immunological markers (PD-L1) in tissues or cells has led to targeted treatment for patients presenting with late stage or metastatic lung cancer. These biomarkers can be detected by immunohistochemistry (IHC) and/or by molecular biology (MB) techniques. These approaches are often complementary but depending on, the quantity and quality of the biological material, the urgency to get the results, the access to technological platforms, the financial resources and the expertise of the team, the choice of the approach can be questioned. The possibility of detecting simultaneously several molecular targets, and of analyzing the degree of tumor mutation burden and of the micro-satellite instability, as well as the recent requirement to quantify the expression of PD-L1 in tumor cells, has led to case by case development of algorithms and international recommendations, which depend on the quality and quantity of biological samples. This review will highlight the different predictive biomarkers detected by IHC for treatment of lung cancer as well as the present advantages and limitations of this approach. A number of perspectives will be considered.
Keywords: immune-oncology; immunocytochemistry; immunohistochemistry; lung cancer; predictive biomarkers.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Hoseok I., Cho J.Y. Lung Cancer Biomarkers. Adv. Clin. Chem. 2015;72:107–170. - PubMed
-
- Aisner D.L., Sholl L.M., Berry L., Rossi M., Chen H., Fujimoto J., Moreira A.L., Ramalingam S., Villaruz L.C., Otterson G.A., et al. The Impact of Smoking and TP53 mutations in lung adenocarcinoma patients with targetable mutations—The Lung Cancer Mutation Consortium (LCMC2) Clin. Cancer Res. 2018;24:1038–1047. doi: 10.1158/1078-0432.CCR-17-2289. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
