

Calibration of Minimally Invasive Continuous Glucose Monitoring Sensors: State-of-The-Art and Current Perspectives
- PMID: 29534053
- PMCID: PMC5872072
- DOI: 10.3390/bios8010024
Calibration of Minimally Invasive Continuous Glucose Monitoring Sensors: State-of-The-Art and Current Perspectives
Abstract
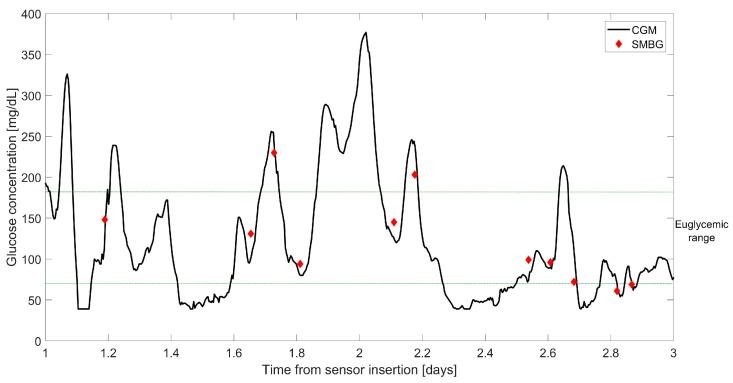
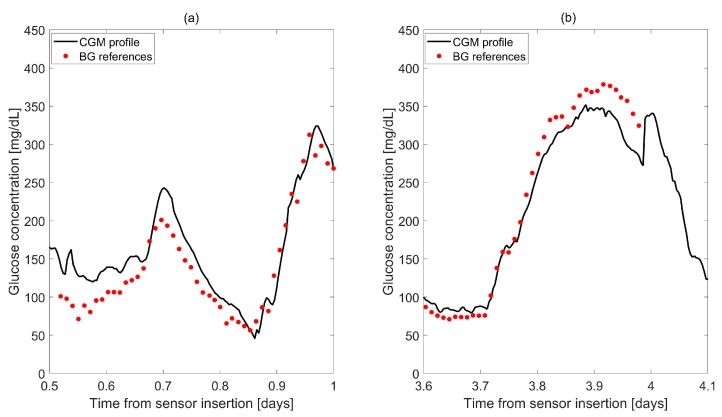
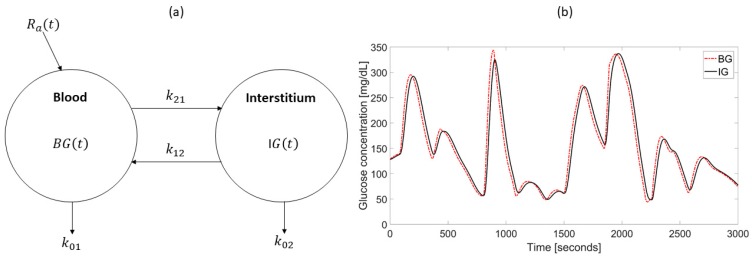
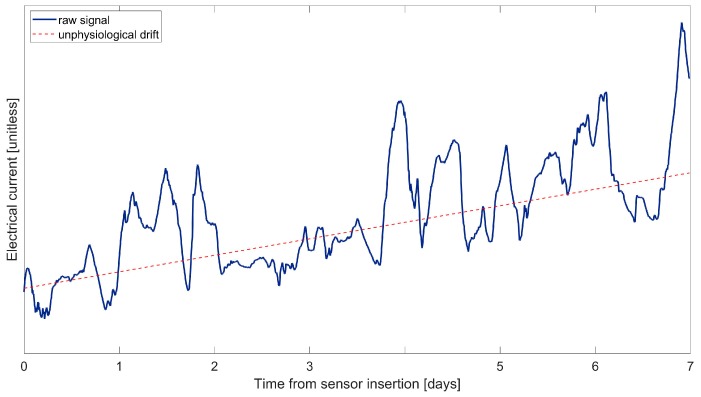
Minimally invasive continuous glucose monitoring (CGM) sensors are wearable medical devices that provide real-time measurement of subcutaneous glucose concentration. This can be of great help in the daily management of diabetes. Most of the commercially available CGM devices have a wire-based sensor, usually placed in the subcutaneous tissue, which measures a "raw" current signal via a glucose-oxidase electrochemical reaction. This electrical signal needs to be translated in real-time to glucose concentration through a calibration process. For such a scope, the first commercialized CGM sensors implemented simple linear regression techniques to fit reference glucose concentration measurements periodically collected by fingerprick. On the one hand, these simple linear techniques required several calibrations per day, with the consequent patient's discomfort. On the other, only a limited accuracy was achieved. This stimulated researchers to propose, over the last decade, more sophisticated algorithms to calibrate CGM sensors, resorting to suitable signal processing, modelling, and machine-learning techniques. This review paper will first contextualize and describe the calibration problem and its implementation in the first generation of CGM sensors, and then present the most recently-proposed calibration algorithms, with a perspective on how these new techniques can influence future CGM products in terms of accuracy improvement and calibration reduction.
Keywords: calibration; continuous glucose monitoring; diabetes; glucose sensors.
Conflict of interest statement
The founding sponsors had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- World Health Organization (WHO) Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications. WHO; Geneva, Switzerland: 1999.
-
- Van Dijk H.W., Verbraak F.D., Fok P.H., Garvin M.K., Sonka M., Lee K., De Vries J.H., Michels R.P., Van Velthoven M.E., Schlingemann R.O., et al. Decreased retinal ganglion cell layer thickness in patients with type 1 diabetes. Investig. Ophthalmol. Vis. Sci. 2010;51:3660–3665. doi: 10.1167/iovs.09-5041. - DOI - PMC - PubMed
-
- Vriesendorp T.M., De Vries J.H., Van Santen S., Moeniralam H.S., De Jonge E., Roos Y.B., Schults M.J., Rosendaal F.R., Hoekstra J.B. Evaluation of short-term consequences of hypoglycemia in an intensive care unit. Crit. Care Med. 2006;34:2714–2718. doi: 10.1097/01.CCM.0000241155.36689.91. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
