

The Renal Elimination Pathways of the Dabigatran Reversal Agent Idarucizumab and its Impact on Dabigatran Elimination
- PMID: 29534609
- PMCID: PMC6714879
- DOI: 10.1177/1076029618755947
The Renal Elimination Pathways of the Dabigatran Reversal Agent Idarucizumab and its Impact on Dabigatran Elimination
Abstract
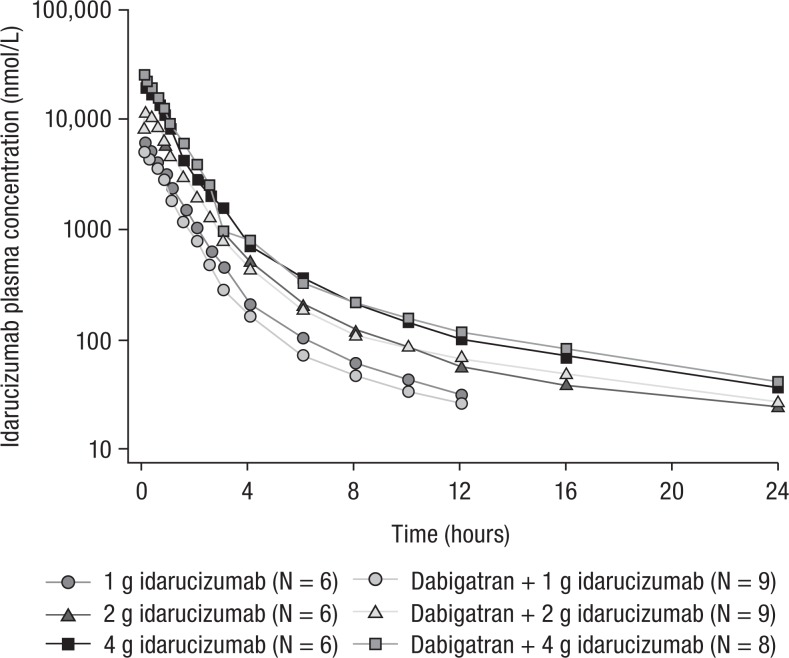
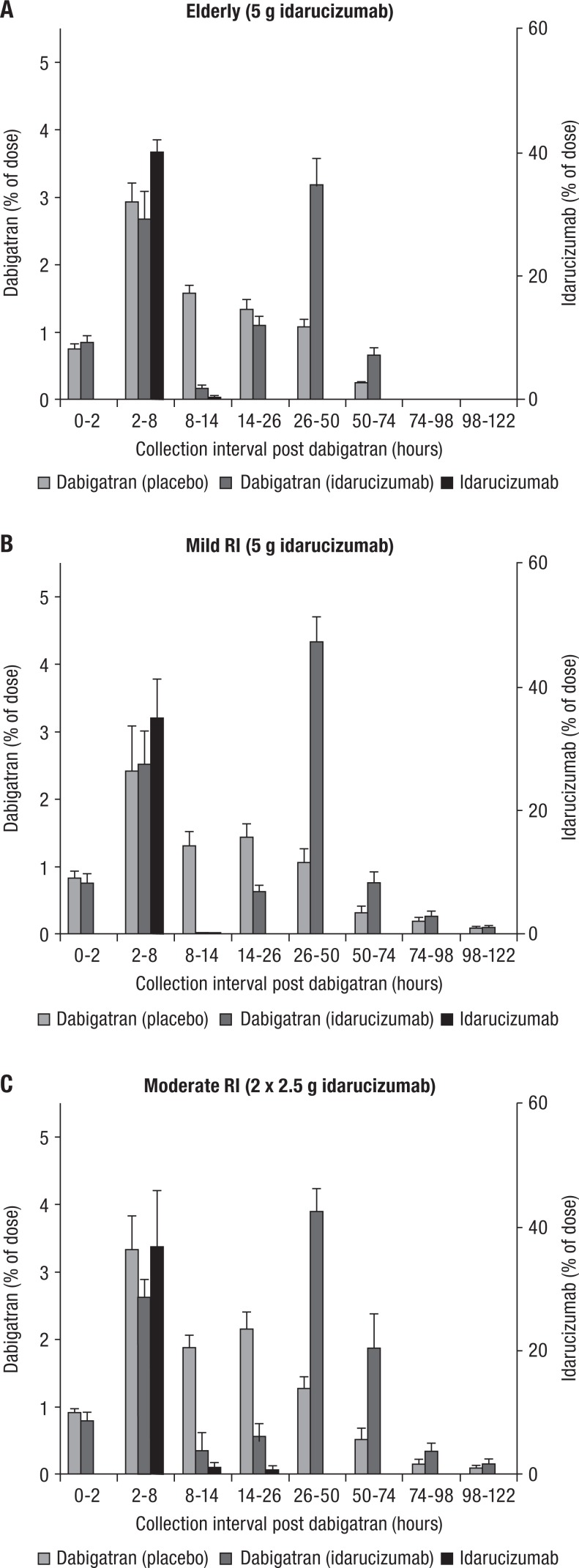
Idarucizumab, a humanized monoclonal antibody fragment (Fab), provides rapid and sustained reversal of dabigatran-mediated anticoagulation. Idarucizumab and dabigatran are mainly eliminated via the kidneys. This analysis aimed to characterize the renal elimination of idarucizumab and investigate the influence of idarucizumab on the pharmacokinetics (PK) of dabigatran and vice versa. Studies were conducted in 5/6 nephrectomized rats, in human volunteers with and without renal impairment, and in a porcine liver trauma model. In both rats and humans, renal impairment increased idarucizumab exposure and initial half-life but did not affect its terminal half-life. Urinary excretion of unchanged idarucizumab increased with increasing idarucizumab dose, suggesting saturation of renal tubular reuptake processes at higher doses. The PK of idarucizumab was unaffected by dabigatran. In contrast, idarucizumab administration resulted in redistribution of dabigatran to the plasma, where it was bound and inactivated by idarucizumab. Urinary excretion of dabigatran after administration of idarucizumab was delayed, but total dabigatran excreted in urine was unaffected. Idarucizumab and dabigatran were eliminated together via renal pathways.
Keywords: clinical pharmacokinetics; elimination; renal clearance.
Conflict of interest statement
Figures





References
-
- Pradaxa. Summary of product characteristics. Boehringer Ingelheim. http://www.medicines.org.uk/emc/medicine/24839. Updated October 19, 2017. Accessed November 23, 2017.
-
- Schulman S, Kearon C, Kakkar AK, et al. ; RE-COVER Study Group. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med. 2009;361(24):2342–2352. - PubMed
-
- Schulman S, Kearon C, Kakkar AK, et al. ; RE-MEDY Trial Investigators; RE-SONATE Trial Investigators. Extended use of dabigatran, warfarin, or placebo in venous thromboembolism. N Engl J Med. 2013;368(8):709–718. - PubMed
-
- Schulman S, Kakkar AK, Goldhaber SZ, et al. ; RE-COVER II Trial Investigators. Treatment of acute venous thromboembolism with dabigatran or warfarin and pooled analysis. Circulation. 2014;129(7):764–772. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
