

Performance of a brief geriatric evaluation compared to a comprehensive geriatric assessment for detection of geriatric syndromes in family medicine: a prospective diagnostic study
- PMID: 29534680
- PMCID: PMC5850979
- DOI: 10.1186/s12877-018-0761-z
Performance of a brief geriatric evaluation compared to a comprehensive geriatric assessment for detection of geriatric syndromes in family medicine: a prospective diagnostic study
Abstract
Background: Geriatric syndromes are rarely detected in family medicine. Within the AGE program (active geriatric evaluation), a brief assessment tool (BAT) designed for family physicians (FP) was developed and its diagnostic performance estimated by comparison to a comprehensive geriatric assessment.
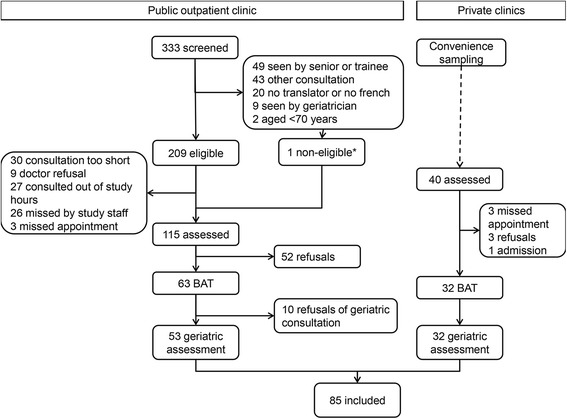
Methods: This prospective diagnostic study was conducted in four primary care sites in Switzerland. Participants were aged at least 70 years and attending a routine appointment with their physician, without previous documented geriatric assessment. Participants were assessed by their family physicians using the BAT, and by a geriatriciant who performed a comprehensive geriatric assessment within the following two-month period (reference standard). Both the BAT and the full assessment targeted eight geriatric syndromes: cognitive impairment, mood impairment, urinary incontinence, visual impairment, hearing loss, undernutrition, osteoporosis and gait and balance impairment. Diagnostic accuracy of the BAT was estimated in terms of sensitivity, specificity, and predictive values; secondary outcomes were measures of feasibility, in terms of added consultation time and comprehensiveness in applying the BAT items.
Results: Prevalence of the geriatric syndromes in participants (N=85, 46 (54.1%) women, mean age 78 years (SD 6))ranged from 30.0% (malnutrition and cognitive impairment) to 71.0% (visual impairment), with a median number of 3 syndromes (IQR 2 to 4) per participant. Sensitivity of the BAT ranged from 25.0% for undernutrition (95%CI 9.8% - 46.7%) to 82.1% for hearing impairment (95%CI 66.5% - 92.5%), while specificity ranged from 45.8% for visual impairment (95%CI 25.6-67.2) to 87.7% for undernutrition (76.3% to 94.9%). Finally, most negative predictive values (NPV) were between 73.5% and 84.1%, excluding visual impairment with a NPV of 50.0%. Family physicians reported BAT use as per instructions for 76.7% of the syndromes assessed.
Conclusions: Although the BAT does not replace a comprehensive geriatric assessment, it is a useful and appropriate tool for the FP to screen elderly patients for most geriatric syndromes.
Trial registration: The study was registered on ClinicalTrials.gov on February 20, 2013 ( NCT01816087 ).
Keywords: Brief geriatric evaluation; Diagnosis; Family medicine; Geriatric syndrome.
Conflict of interest statement
Ethics approval and consent to participate
The study was conducted in accordance with the Declaration of Helsinki. Patients gave written informed consent. The study was approved on the 19th of October 2012 by the Research Ethics Commission of the Canton of Vaud, Switzerland (number 287/2012), and registered on ClinicalTrials.gov (number NCT01816087).
Consent for publication
Not applicable.
Competing interests
All authors have completed the ICMJE uniform disclosure form at
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
A prospective study assessing agreement and reliability of a geriatric evaluation.BMC Geriatr. 2017 Jul 19;17(1):153. doi: 10.1186/s12877-017-0546-9. BMC Geriatr. 2017. PMID: 28724392 Free PMC article.
-
[Seven questions for elderly in the practice of primary care physicians].Adv Gerontol. 2017;30(2):231-235. Adv Gerontol. 2017. PMID: 28575562 Russian.
-
Geriatric assessment tools.Mt Sinai J Med. 2011 Jul-Aug;78(4):489-97. doi: 10.1002/msj.20277. Mt Sinai J Med. 2011. PMID: 21748738 Review.
-
Screening for common problems in ambulatory elderly: clinical confirmation of a screening instrument.Am J Med. 1996 Apr;100(4):438-43. doi: 10.1016/S0002-9343(97)89520-4. Am J Med. 1996. PMID: 8610731
-
Geriatric syndromes and assessment in older cancer patients.Oncology (Williston Park). 2001 Dec;15(12):1567-77, 1580; discussion 1581, 1586, 1591. Oncology (Williston Park). 2001. PMID: 11780701 Review.
Cited by
-
Multidimensional Geriatric Assessment with MAGIC Questionnaire and Quality of Life in Elderly Primary Care Patients.Int J Environ Res Public Health. 2020 Sep 28;17(19):7089. doi: 10.3390/ijerph17197089. Int J Environ Res Public Health. 2020. PMID: 32998200 Free PMC article.
-
Developing a Delphi Consensus on the Domains and Conduct of Brief Geriatric Assessments in Singapore.Ann Geriatr Med Res. 2025 Jun;29(2):177-184. doi: 10.4235/agmr.24.0198. Epub 2025 Feb 19. Ann Geriatr Med Res. 2025. PMID: 39967564 Free PMC article.
-
The relationship between accelerometer-based physical activity, sedentary behavior, and seven common geriatric syndromes: a two-sample Mendelian randomization study.Front Public Health. 2024 Aug 5;12:1406303. doi: 10.3389/fpubh.2024.1406303. eCollection 2024. Front Public Health. 2024. PMID: 39161855 Free PMC article.
-
Application and implementation of brief geriatric assessment in primary care and community settings: a scoping review.BMC Geriatr. 2025 Jan 2;25(1):2. doi: 10.1186/s12877-024-05615-9. BMC Geriatr. 2025. PMID: 39748279 Free PMC article.
-
Rapid Geriatric Assessment, Physical Activity, and Sleep Quality in Adults Aged more than 65 Years: A Preliminary Study.J Nutr Health Aging. 2019;23(7):617-622. doi: 10.1007/s12603-019-1212-z. J Nutr Health Aging. 2019. PMID: 31367725 Free PMC article.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
