

Interventional bronchoscopy in malignant central airway obstruction by extra-pulmonary malignancy
- PMID: 29534706
- PMCID: PMC5851311
- DOI: 10.1186/s12890-018-0608-6
Interventional bronchoscopy in malignant central airway obstruction by extra-pulmonary malignancy
Abstract
Background: Interventional bronchoscopy is considered an effective treatment option for malignant central airway obstruction (MCAO). However, there are few reports of interventional bronchoscopy in patients with MCAOs due to extra-pulmonary malignancy. Therefore, the objective of this study was to investigate treatment outcomes and prognostic factors for bronchoscopic intervention in patients with MCAO due to extra-pulmonary malignancy.
Methods: We retrospectively analyzed consecutive 98 patients with MCAO due to extra-pulmonary malignancy who underwent interventional bronchoscopy between 2004 and 2014 at Samsung Medical Center (Seoul, Korea).
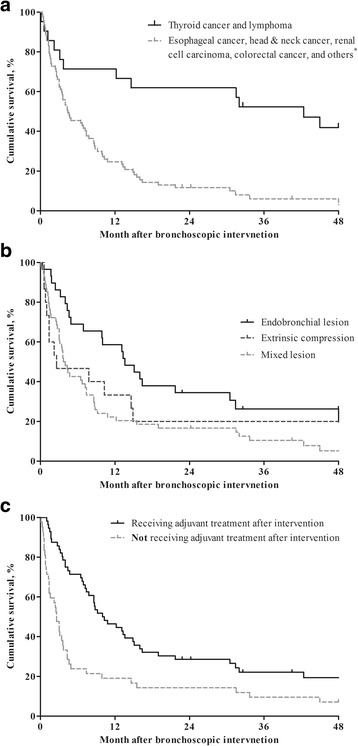
Results: The most common primary site of malignancy was esophageal cancer (37.9%), followed by thyroid cancer (16.3%) and head & neck cancer (10.2%). Bronchoscopic interventions were usually performed using a combination of mechanical debulking (84.7%), stent insertion (70.4%), and laser cauterization (37.8%). Of 98 patients, 76 (77.6%) patients had MCAO due to progression of malignancy, and 42 (42.9%) patients had exhausted all other anti-cancer treatment at the time of bronchoscopic intervention. Technical success was achieved in 89.9% of patients, and acute complications and procedure-related deaths occurred in 20.4% and 3.1% of patients, respectively. Reduced survival was associated with MCAO due to cancer other than thyroid cancer or lymphoma, mixed lesions, and not receiving adjuvant treatment after bronchoscopic intervention.
Conclusions: Bronchoscopic intervention could be a safe and effective procedure for MCAO due to end-stage extra-pulmonary malignancies. In addition, we identified possible prognostic factors for poor survival after intervention, which could guide clinicians select candidates that will benefit from bronchoscopic intervention.
Keywords: Extra-pulmonary malignancy; Interventional bronchoscopy; Malignant central airway obstruction.
Conflict of interest statement
Ethics approval and consent to participate
This study obtained approval from the institutional review board (IRB no. 2017-01-033) to review and publish information obtained from patient records. The need for informed consent was waived because patient information was anonymized and de-identified prior to analysis.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Ost DE, Ernst A, Grosu HB, Lei X, Diaz-Mendoza J, Slade M, Gildea TR, Machuzak MS, Jimenez CA, Toth J, et al. Therapeutic bronchoscopy for malignant central airway obstruction: success rates and impact on dyspnea and quality of life. Chest. 2015;147(5):1282–1298. doi: 10.1378/chest.14-1526. - DOI - PMC - PubMed
-
- Nihei K, Ishikura S, Kawashima M, Ogino T, Ito Y, Ikeda H. Short-course palliative radiotherapy for airway stenosis in non-small cell lung cancer. Int J Clin Oncol. 2002;7(5):284–288. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
