

The efficacy and safety of pre-hospital cooling after out-of-hospital cardiac arrest: a systematic review and meta-analysis
- PMID: 29534742
- PMCID: PMC5850970
- DOI: 10.1186/s13054-018-1984-2
The efficacy and safety of pre-hospital cooling after out-of-hospital cardiac arrest: a systematic review and meta-analysis
Abstract
Background: Mild therapeutic hypothermia (TH), or targeted temperature management, improves survival and neurological outcomes in patients after out-of-hospital cardiac arrest (OHCA). International guidelines strongly support initiating TH for all eligible individuals presenting with OHCA; however, the timing of cooling initiation remains uncertain. This systematic review and meta-analysis was conducted with all available randomised controlled trials (RCTs) included to explore the efficacy and safety of initiating pre-hospital TH in patients with OHCA.
Methods: The MEDLINE and Cochrane databases were searched from inception to October 2017. Inclusion criteria for full-text review included RCTs comparing pre-hospital TH with no pre-hospital TH after cardiac arrest, patients > 14 years of age with documented cardiac arrest from any rhythm, and outcome data that included survival to hospital discharge and temperature at hospital arrival. Results of retrieved studies were compared through meta-analysis using random effects modelling.
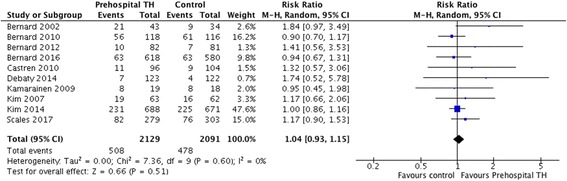
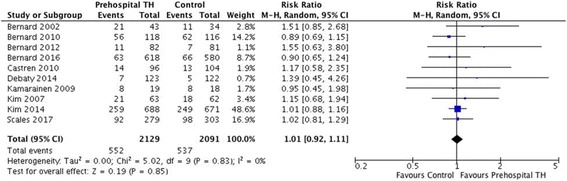
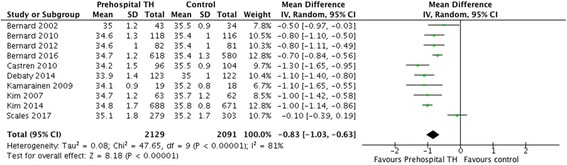
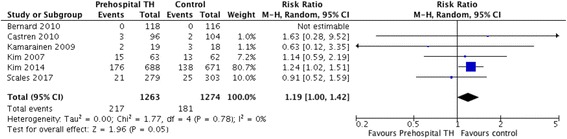
Results: A total of 10 trials comprising 4220 patients were included. There were no significant differences between the two arms for the primary outcome of neurological recovery (risk ratio [RR] 1.04, 95% CI 0.93-1.15) or the secondary outcome of survival to hospital discharge (RR 1.01, 95% CI 0.92-1.11). However, there was a significantly lower temperature at hospital arrival in patients receiving pre-hospital TH (mean difference - 0.83, 95% CI - 1.03 to - 0.63). Pre-hospital TH significantly increased the risk of re-arrest (RR 1.19, 95% CI 1.00 to 1.41). No survival differences were observed among subgroups of patients who received intra-arrest TH vs post-arrest TH or who had shockable vs non-shockable rhythms.
Conclusions: Pre-hospital TH after OHCA effectively decreases body temperature at the time of hospital arrival. However, it does not improve rates of survival with good neurological outcome or overall survival and is associated with increased rates of re-arrest.
Keywords: Cooling; Out-of-hospital cardiac arrest; Pre-hospital; Therapeutic hypothermia.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Howes D, Gray SH, Brooks SC, Boyd JG, Djogovic D, Golan E, Green RS, Jacka MJ, Sinuff T, Chaplin T, et al. Canadian guidelines for the use of targeted temperature management (therapeutic hypothermia) after cardiac arrest: a joint statement from the Canadian Critical Care Society (CCCS), Canadian Neurocritical Care Society (CNCCS), and the Canadian Critical Care Trials Group (CCCTG) Resuscitation. 2016;98:48–63. doi: 10.1016/j.resuscitation.2015.07.052. - DOI - PubMed
-
- Nikolaou NI, Arntz HR, Bellou A, Beygui F, Bossaert LL, Cariou A, Initial management of acute coronary syndromes section Collaborator European Resuscitation Council Guidelines for Resuscitation 2015 Section 8. Initial management of acute coronary syndromes. Resuscitation. 2015;95:264–277. doi: 10.1016/j.resuscitation.2015.07.030. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
