

Geographic variation in the provider of screening colonoscopy in Canada: a population-based cohort study
- PMID: 29535104
- PMCID: PMC5878955
- DOI: 10.9778/cmajo.20170131
Geographic variation in the provider of screening colonoscopy in Canada: a population-based cohort study
Abstract
Background: Screening colonoscopy for the detection of colorectal carcinoma is provided by several specialties. Few studies have assessed geographic variation in the delivery of this care. Our objective was to investigate how geographic and socioeconomic factors affect who provides screening colonoscopy in Canada.
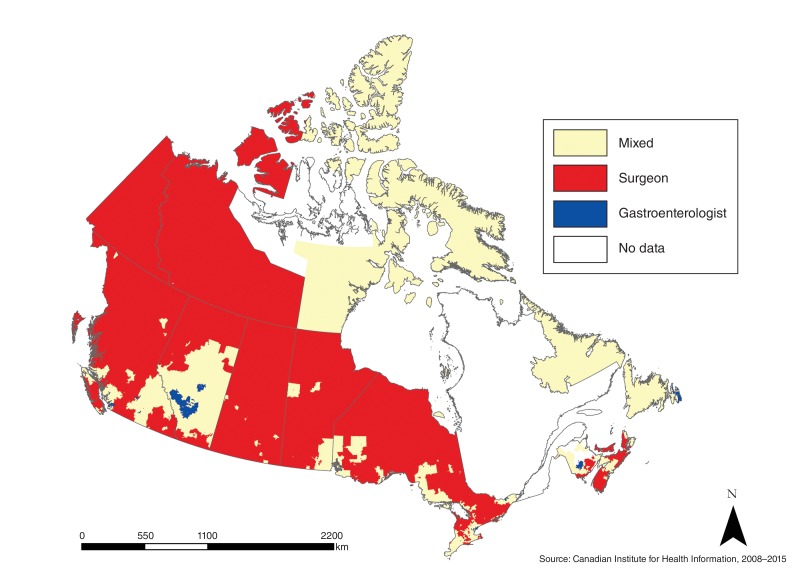
Methods: This was a population-based cohort of all screening colonoscopy procedures performed at publicly funded Canadian health care facilities (excluding those in Quebec) between April 2008 and March 2015. The main outcome of interest was the proportion of colonoscopy procedures performed by surgeons versus gastroenterologists at the neighbourhood level. Predictors of interest included socioeconomic and geographic variables. We used spatial analysis to evaluate significant clustering of practitioner services and multinomial logistic regression to model predictors.
Results: We identified 658 113 screening colonoscopy procedures performed by 1886 providers (1169 surgeons and 717 gastroenterologists) over the study period, of which 353 165 (53.7%) were performed by surgeons. A total of 24.2% of neighbourhoods were located within clusters predominantly served by gastroenterologists, and 19.5% were within surgeon clusters; the remainder were in mixed clusters. Rural neighbourhoods had a significantly increased relative risk of being within a surgeon cluster (relative risk [RR] 5.38, 95% confidence interval [CI] 3.48-8.01) compared to mixed clusters and nearly 100 times higher relative risk of being in a surgeon cluster compared to gastroenterologist clusters (RR 98.95, 95% CI 15.3-427.2). Neighbourhoods with the highest socioeconomic status were 1.74 (95% CI 1.14-2.56) times likelier to be in gastroenterologist clusters than in mixed clusters.
Interpretation: Surgeons provide a large proportion of colonoscopy procedures in Canada and are essential for access to care, particularly in rural regions. Most Canadians are served relatively equally by surgeons and gastroenterologists. This emphasizes the importance of both specialties to the delivery of colonoscopy care across the country.
Copyright 2018, Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Geographic distribution of colonoscopy providers in the United States: An analysis of medicare claims data.Surg Endosc. 2022 Oct;36(10):7673-7678. doi: 10.1007/s00464-022-09083-3. Epub 2022 Jun 21. Surg Endosc. 2022. PMID: 35729404
-
Geographic and socioeconomic factors affecting delivery of bariatric surgery across high- and low-utilization healthcare systems.Br J Surg. 2017 Jun;104(7):891-897. doi: 10.1002/bjs.10517. Epub 2017 Apr 4. Br J Surg. 2017. PMID: 28376245
-
Rural-Urban Differences in Access to Specialist Providers of Colorectal Cancer Care in the United States: A Physician Workforce Issue.JAMA Surg. 2014 Jun;149(6):537-43. doi: 10.1001/jamasurg.2013.5062. JAMA Surg. 2014. PMID: 24740165
-
Quality measures for colonoscopy: where should we be in 2015?Curr Gastroenterol Rep. 2015 Mar;17(3):10. doi: 10.1007/s11894-015-0432-6. Curr Gastroenterol Rep. 2015. PMID: 25740247 Review.
-
[Quality is the Key for Emerging Issues of Population-based Colonoscopy Screening].Korean J Gastroenterol. 2018 Jan 25;71(1):3-9. doi: 10.4166/kjg.2018.71.1.3. Korean J Gastroenterol. 2018. PMID: 29361807 Review. Korean.
Cited by
-
Evaluation of the quality of colonoscopies performed by Alberta North Zone surgeons, family physicians and internists: a quality improvement initiative.CMAJ Open. 2023 Aug 1;11(4):E654-E661. doi: 10.9778/cmajo.20210237. Print 2023 Jul-Aug. CMAJ Open. 2023. PMID: 37527900 Free PMC article.
-
General surgery in Canada: current scope of practice and future needs.Can J Surg. 2020 Sep-Oct;63(5):E396-E408. doi: 10.1503/cjs.004419. Can J Surg. 2020. PMID: 33009899 Free PMC article.
-
Canadian considerations on updating the age of initiation for colorectal cancer screening in individuals at average risk.Can J Surg. 2025 Aug 8;68(4):E313-E324. doi: 10.1503/cjs.000825. Print 2025 Jul-Aug. Can J Surg. 2025. PMID: 40780872 Free PMC article. Review.
-
Provision of colonoscopy in rural settings: A qualitative assessment of provider context, barriers, facilitators, and capacity.J Rural Health. 2024 Mar;40(2):272-281. doi: 10.1111/jrh.12793. Epub 2023 Sep 7. J Rural Health. 2024. PMID: 37676061 Free PMC article.
References
-
- Arnold M, Sierra MS, Laversanne M, et al. Global patterns and trends in colorectal cancer incidence and mortality. Gut. 2017;66:683–91. - PubMed
-
- Muto T, Bussey HJ, Morson BC. The evolution of cancer of the colon and rectum. Cancer. 1975;36:2251–70. - PubMed
-
- Baxter NN, Goldwasser MA, Paszat LF, et al. Association of colonoscopy and death from colorectal cancer. Ann Intern Med. 2009;150:1–8. - PubMed
-
- Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectal cancer by colonoscopic polypectomy. N Engl J Med. 1993;329:1977–81. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous