

Toward dual hematopoietic stem-cell transplantation and solid-organ transplantation for sickle-cell disease
- PMID: 29535106
- PMCID: PMC5851417
- DOI: 10.1182/bloodadvances.2017012500
Toward dual hematopoietic stem-cell transplantation and solid-organ transplantation for sickle-cell disease
Abstract
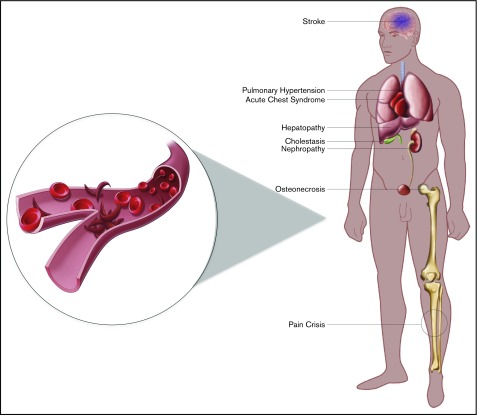
Sickle-cell disease (SCD) leads to recurrent vaso-occlusive crises, chronic end-organ damage, and resultant physical, psychological, and social disabilities. Although hematopoietic stem-cell transplantation (HSCT) is potentially curative for SCD, this procedure is associated with well-recognized morbidity and mortality and thus is ideally offered only to patients at high risk of significant complications. However, it is difficult to identify patients at high risk before significant complications have occurred, and once patients experience significant organ damage, they are considered poor candidates for HSCT. In turn, patients who have experienced long-term organ toxicity from SCD such as renal or liver failure may be candidates for solid-organ transplantation (SOT); however, the transplanted organs are at risk of damage by the original disease. Thus, dual HSCT and organ transplantation could simultaneously replace the failing organ and eliminate the underlying disease process. Advances in HSCT conditioning such as reduced-intensity regimens and alternative donor selection may expand both the feasibility of and potential donor pool for transplantation. This review summarizes the current state of HSCT and organ transplantation in SCD and discusses future directions and the clinical feasibility of dual HSCT/SOT.
© 2018 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
Similar articles
-
Hematopoietic stem cell transplantation for sickle cell disease: current practice and emerging trends.Hematology Am Soc Hematol Educ Program. 2011;2011:273-9. doi: 10.1182/asheducation-2011.1.273. Hematology Am Soc Hematol Educ Program. 2011. PMID: 22160045 Review.
-
Hematopoietic stem cell transplantation for sickle cell disease: Progress and challenges.Pediatr Blood Cancer. 2018 Sep;65(9):e27263. doi: 10.1002/pbc.27263. Epub 2018 May 24. Pediatr Blood Cancer. 2018. PMID: 29797658 Review.
-
Hematopoietic Stem Cell Transplant for Sickle Cell Disease: PATIENT SELEction and Timing Based on Sickle Cell-Related Multiple Chronic Conditions.Cell Transplant. 2021 Jan-Dec;30:9636897211046559. doi: 10.1177/09636897211046559. Cell Transplant. 2021. PMID: 34628962 Free PMC article.
-
Hematopoietic Stem Cell Transplantation in Sickle Cell Disease: A Multidimentional Review.Cell Transplant. 2024 Jan-Dec;33:9636897241246351. doi: 10.1177/09636897241246351. Cell Transplant. 2024. PMID: 38680015 Free PMC article. Review.
-
Hematopoietic stem cell transplantation for sickle cell disease: The changing landscape.Hematol Oncol Stem Cell Ther. 2017 Dec;10(4):259-266. doi: 10.1016/j.hemonc.2017.05.008. Epub 2017 Jun 15. Hematol Oncol Stem Cell Ther. 2017. PMID: 28641096 Review.
Cited by
-
The Role of CTLA4 and Its Polymorphisms in Solid Organ and Haematopoietic Stem Cell Transplantation.Int J Mol Sci. 2021 Mar 17;22(6):3081. doi: 10.3390/ijms22063081. Int J Mol Sci. 2021. PMID: 33802937 Free PMC article. Review.
-
Management of Sickle Cell Intrahepatic Cholestasis: An Argument in Favor of Automated Exchange Transfusion.Clin Hematol Int. 2019 Sep 1;1(3):127-133. doi: 10.2991/chi.d.190630.001. eCollection 2019 Sep. Clin Hematol Int. 2019. PMID: 34595422 Free PMC article.
-
Haplo-stem cell transplant post liver transplantation to cure sickle cell disease with related liver dysfunction: a case series.Commun Med (Lond). 2025 Aug 15;5(1):354. doi: 10.1038/s43856-025-01040-0. Commun Med (Lond). 2025. PMID: 40817313 Free PMC article.
-
Tandem Orthotopic Living Donor Liver Transplantation Followed by Same Donor Haploidentical Hematopoietic Stem Cell Transplantation for DOCK8 Deficiency.Transplantation. 2019 Oct;103(10):2144-2149. doi: 10.1097/TP.0000000000002649. Transplantation. 2019. PMID: 30720689 Free PMC article.
-
Emerging need for a hepato-hematology program for patients with sickle cell disease in Saudi Arabia.Saudi J Gastroenterol. 2025 Mar 1;31(2):53-58. doi: 10.4103/sjg.sjg_419_24. Epub 2025 Mar 7. Saudi J Gastroenterol. 2025. PMID: 40051245 Free PMC article.
References
-
- Yawn BP, Buchanan GR, Afenyi-Annan AN, et al. . Management of sickle cell disease: summary of the 2014 evidence-based report by expert panel members. JAMA. 2014;312(10):1033-1048. - PubMed
-
- Steinberg MH. Management of sickle cell disease. N Engl J Med. 1999;340(13):1021-1030. - PubMed
-
- Platt OS, Brambilla DJ, Rosse WF, et al. . Mortality in sickle cell disease. Life expectancy and risk factors for early death. N Engl J Med. 1994;330(23):1639-1644. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
