

Biomarkers of Myocardial Fibrosis: Revealing the Natural History of Fibrogenesis in Fabry Disease Cardiomyopathy
- PMID: 29535138
- PMCID: PMC5907540
- DOI: 10.1161/JAHA.117.007124
Biomarkers of Myocardial Fibrosis: Revealing the Natural History of Fibrogenesis in Fabry Disease Cardiomyopathy
Abstract
Background: Cardiomyopathy is a major determinant of overall Fabry disease (FD) prognosis, with the worst outcomes in patients with myocardial fibrosis. Late gadolinium enhancement is currently the gold standard for evaluation of replacement myocardial fibrosis; however, this event is irreversible, thus identification of biomarkers of earlier diffuse fibrosis is paramount.
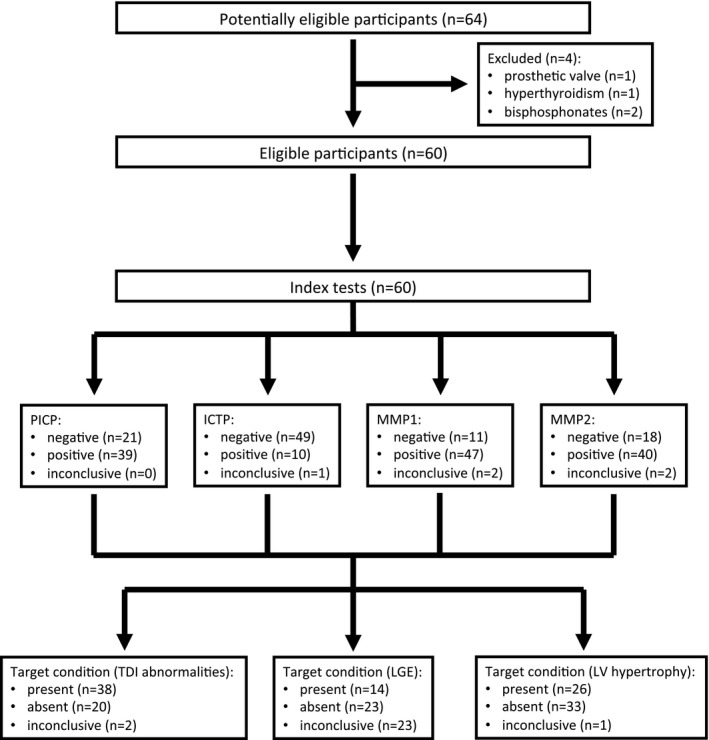
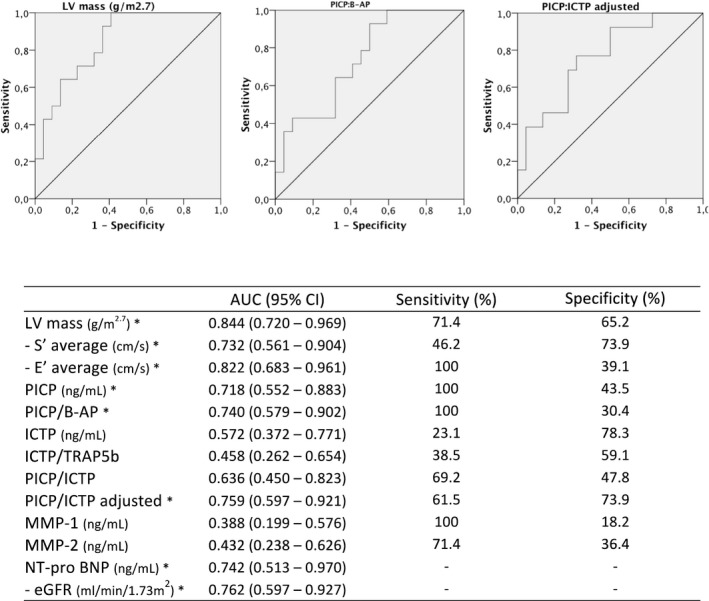
Methods and results: Type I collagen synthesis and degradation biomarkers (PICP [carboxyterminal propeptide of procollagen type I], ICTP [carboxyterminal telopeptide of type I collagen], and MMP1 [matrix metalloproteinase 1] and MMP2) and markers of bone synthesis and degradation were evaluated (to adjust type I collagen metabolism to bone turnover) in FD patients and controls. FD patients were grouped by cardiomyopathy severity, according to echocardiogram: (1) normal, (2) tissue Doppler abnormalities, (3) left ventricular hypertrophy. A significant increase in PICP and a significant decrease in matrix metalloproteinases were observed in FD patients; even the group with normal echocardiogram had a significant increase in PICP. We also found a significant correlation between left ventricular mass and PICP (ρ=0.378, P=0.003) and MMP1 (ρ=-0.484, P<0.001). PICP (adjusted for bone turnover) was the better predictor of left ventricular mass in multivariable regression, and its diagnostic accuracy to predict late gadolinium enhancement was also significant.
Conclusions: Collagen type I synthesis is increased in FD cardiomyopathy, even in the earlier stages of the disease, and this profibrotic state has good predictive value for and is likely to be critical to the development of overt left ventricular hypertrophy. Moreover, inhibition of enzymes involved in collagen type I cleavage also seems crucial to myocardial collagen deposition.
Keywords: Fabry disease cardiomyopathy; biomarkers; carboxyterminal propeptide of procollagen type I; cardiac fibrosis; matrix metalloproteinases.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Mehta A, Clarke JTR, Giugliani R, Elliott P, Linhart A, Beck M, Sunder‐Plassmann G; on behalf of the FOS Investigators . Natural course of Fabry disease: changing pattern of cause of death in FOS—Fabry Outcome Survey. J Med Genet. 2009;46:548–552. - PubMed
-
- Waldek S, Patel MR, Banikazemi M, Lemay R, Lee P. Life expectancy and cause of death in males and females with Fabry disease: findings from the Fabry Registry. Genet Med. 2009;11:790–796. - PubMed
-
- Schiffmann R, Warnock DG, Banikazemi M, Bultas J, Linthorst GE, Packman S, Sorensen SA, Wilcox WR, Desnick RJ. Fabry disease: progression of nephropathy, and prevalence of cardiac and cerebrovascular events before enzyme replacement therapy. Nephrol Dial Transplant. 2009;24:2102–2111. - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
