

Glycosylation Profile of Immunoglobulin G Is Cross-Sectionally Associated With Cardiovascular Disease Risk Score and Subclinical Atherosclerosis in Two Independent Cohorts
- PMID: 29535164
- PMCID: PMC5970566
- DOI: 10.1161/CIRCRESAHA.117.312174
Glycosylation Profile of Immunoglobulin G Is Cross-Sectionally Associated With Cardiovascular Disease Risk Score and Subclinical Atherosclerosis in Two Independent Cohorts
Abstract
Rationale: One measure of protein glycosylation (GlycA) has been reported to predict higher cardiovascular risk by reflecting inflammatory pathways.
Objective: The main objective of this study is to assess the role of a comprehensive panel of IgG glycosylation traits on traditional risk factors for cardiovascular disease and on presence of subclinical atherosclerosis in addition to GlycA.
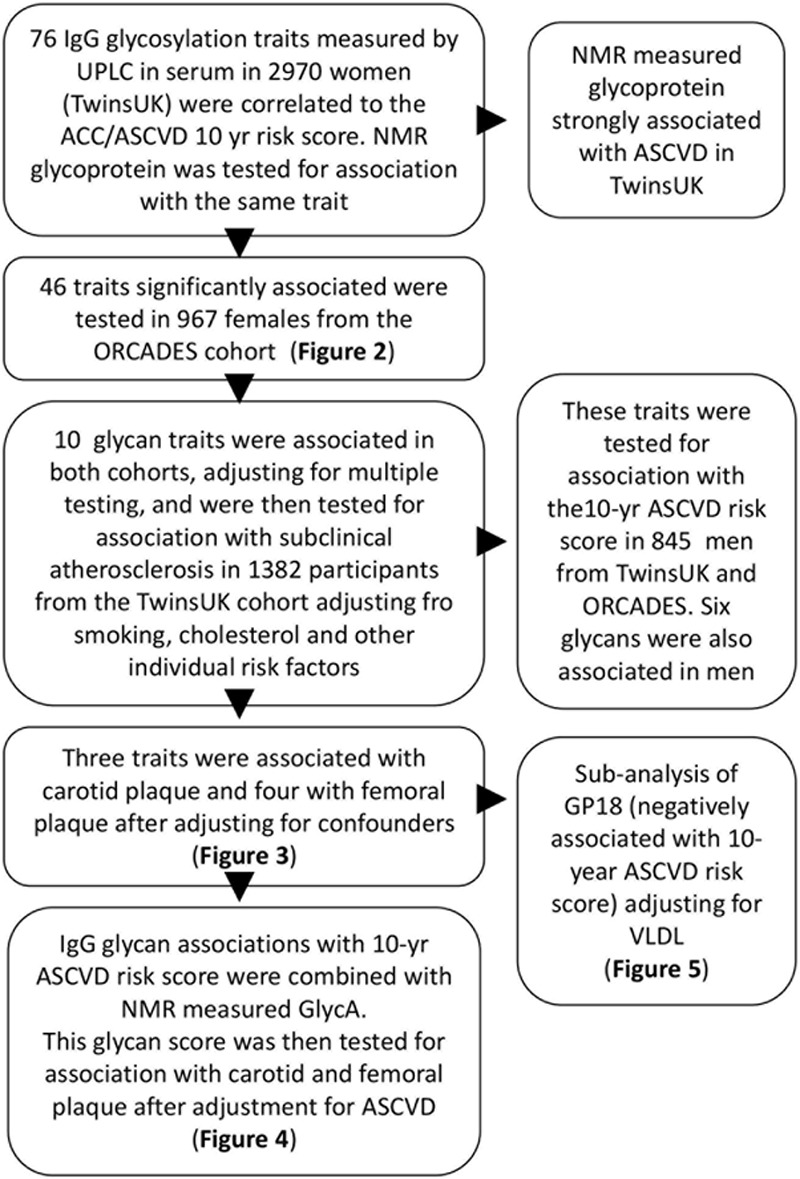
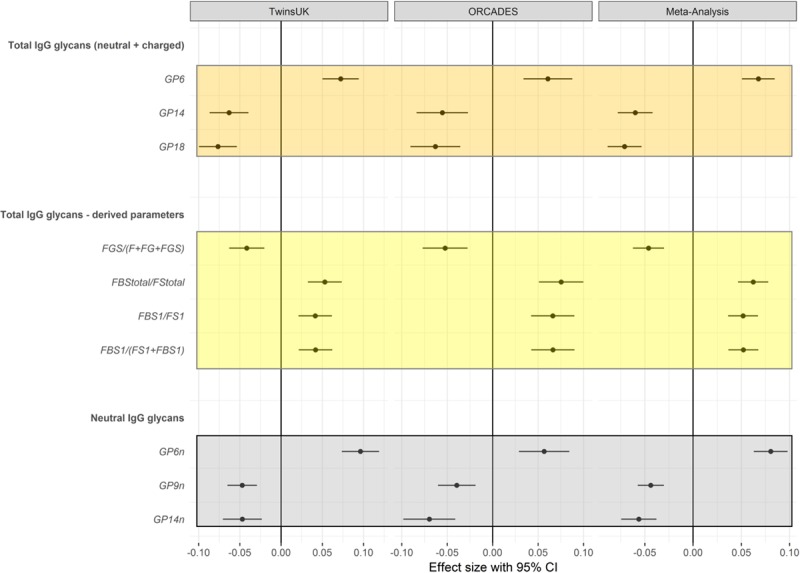
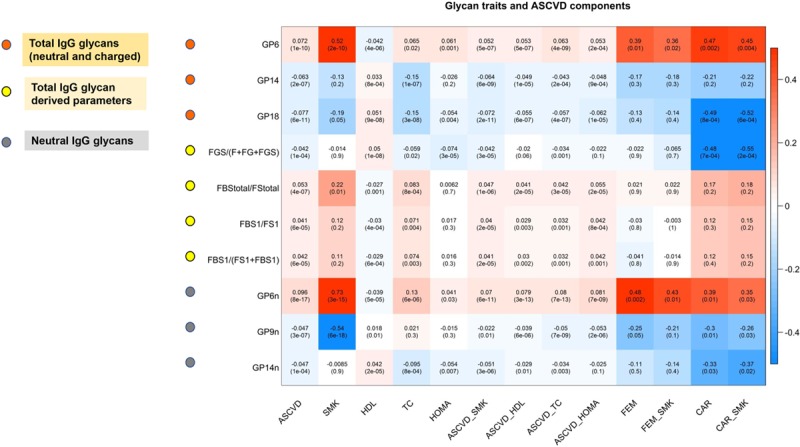
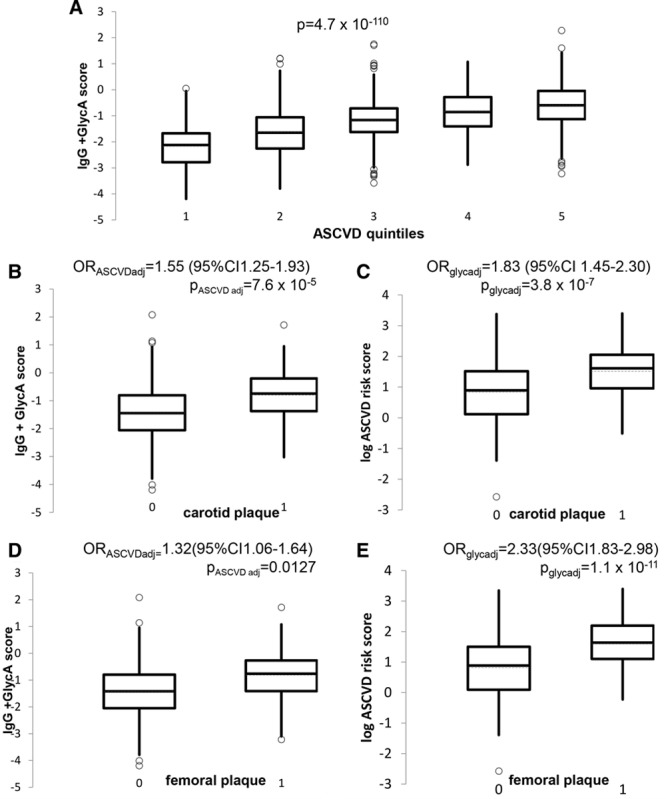
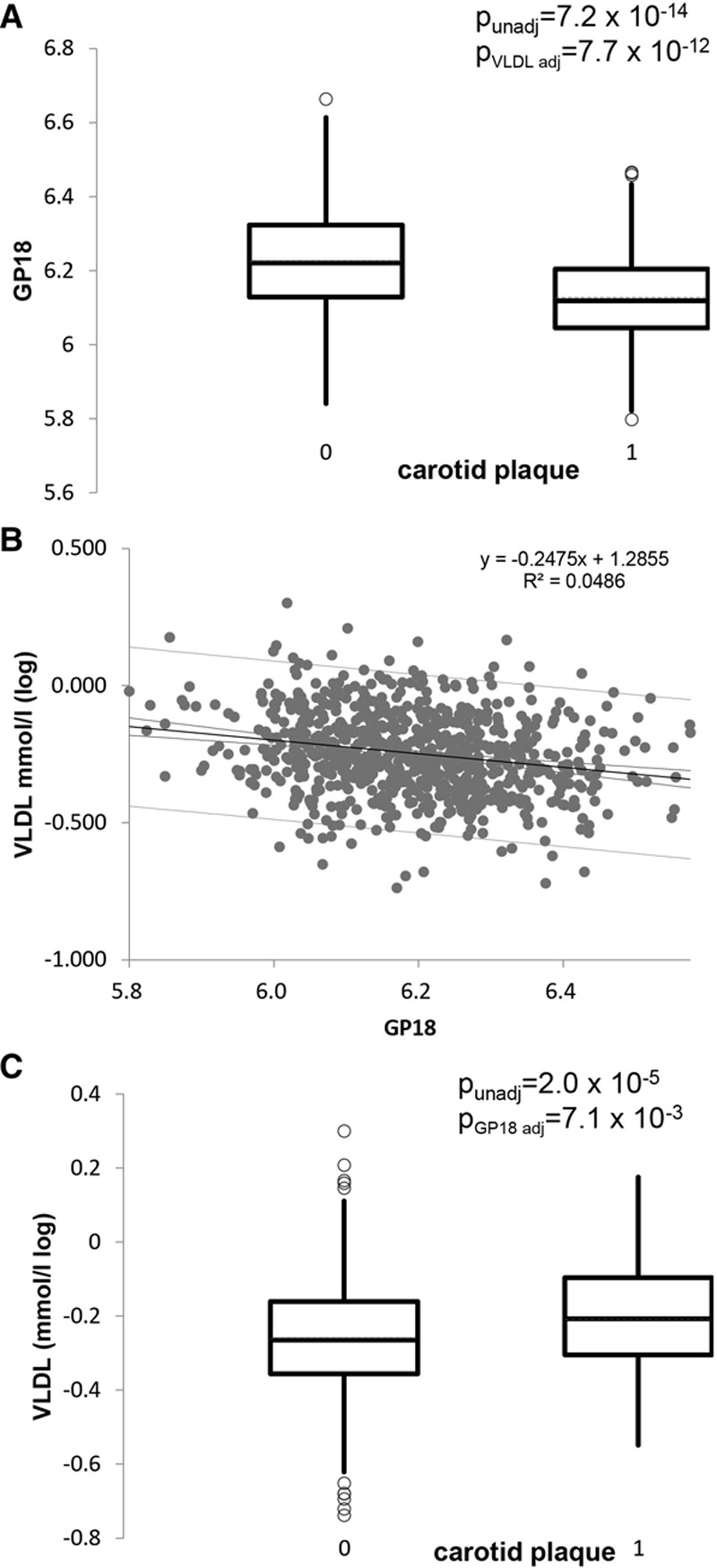
Methods and results: We measured 76 IgG glycosylation traits in 2970 women (age range, 40-79 years) from the TwinsUK cohort and correlated it to their estimated 10-year atherosclerotic cardiovascular disease risk score and their carotid and femoral plaque measured by ultrasound imaging. Eight IgG glycan traits are associated with the 10-year atherosclerotic cardiovascular disease risk score after adjusting for multiple tests and for individual risk factors-5 with increased risk and 3 with decreased risk. These glycans replicated in 967 women from ORCADES cohort (Orkney Complex Disease Study), and 6 of them were also associated in 845 men. A linear combination of IgG glycans and GlycA is also associated with presence of carotid (odds ratio, 1.55; 95% confidence interval, 1.25-1.93; P=7.5×10-5) and femoral (odds ratio, 1.32; 95% confidence interval, 1.06-1.64; P=0.01) plaque in a subset of women with atherosclerosis data after adjustment for traditional risk factors. One specific glycosylation trait, GP18-the percentage of FA2BG2S1 glycan in total IgG glycans, was negatively correlated with very-low-density lipoprotein and triglyceride levels in serum and with presence of carotid plaque (odds ratio, 0.60; 95% confidence interval, 0.50-0.71; P=5×10-4).
Conclusions: We find molecular pathways linking IgG to arterial lesion formation. Glycosylation traits are independently associated with subclinical atherosclerosis. One specific trait related to the sialylated N-glycan is negatively correlated with cardiovascular disease risk, very-low-density lipoprotein and triglyceride serum levels, and presence of carotid plaque.
Keywords: atherosclerosis; cardiovascular disease risk; glycosylation; immunoglobulin G; plaque, atherosclerotic.
© 2018 The Authors.
Figures
Comment in
-
Glycomics and Cardiovascular Disease: Advancing Down the Path Towards Precision.Circ Res. 2018 May 25;122(11):1488-1490. doi: 10.1161/CIRCRESAHA.118.313054. Circ Res. 2018. PMID: 29798896 No abstract available.
References
-
- GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2015;385:117–171. doi: 10.1016/S0140-6736(14)61682-2. - PMC - PubMed
-
- Jackson R, Lawes CM, Bennett DA, Milne RJ, Rodgers A. Treatment with drugs to lower blood pressure and blood cholesterol based on an individual’s absolute cardiovascular risk. Lancet. 2005;365:434–441. doi: 10.1016/S0140-6736(05)17833-7. - PubMed
-
- Ridker PM, Buring JE, Rifai N, Cook NR. Development and validation of improved algorithms for the assessment of global cardiovascular risk in women: the Reynolds Risk Score. JAMA. 2007;297:611–619. doi: 10.1001/jama.297.6.611. - PubMed
-
- Assmann G, Cullen P, Schulte H. Simple scoring scheme for calculating the risk of acute coronary events based on the 10-year follow-up of the prospective cardiovascular Münster (PROCAM) study. Circulation. 2002;105:310–315. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
