

Shared and Distinct Rupture Discriminants of Small and Large Intracranial Aneurysms
- PMID: 29535267
- PMCID: PMC5871584
- DOI: 10.1161/STROKEAHA.117.019929
Shared and Distinct Rupture Discriminants of Small and Large Intracranial Aneurysms
Abstract
Background and purpose: Many ruptured intracranial aneurysms (IAs) are small. Clinical presentations suggest that small and large IAs could have different phenotypes. It is unknown if small and large IAs have different characteristics that discriminate rupture.
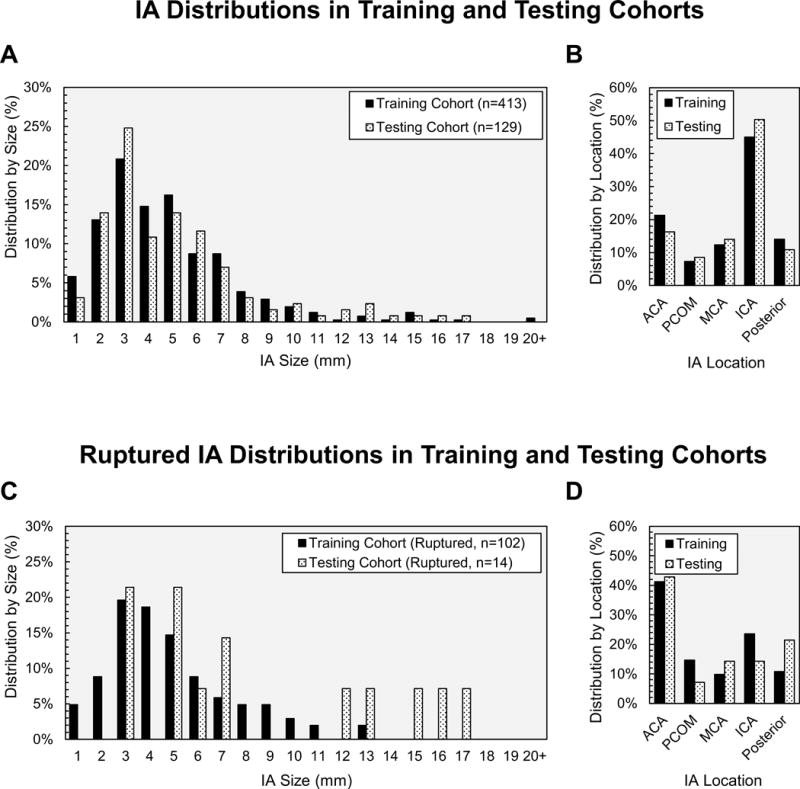
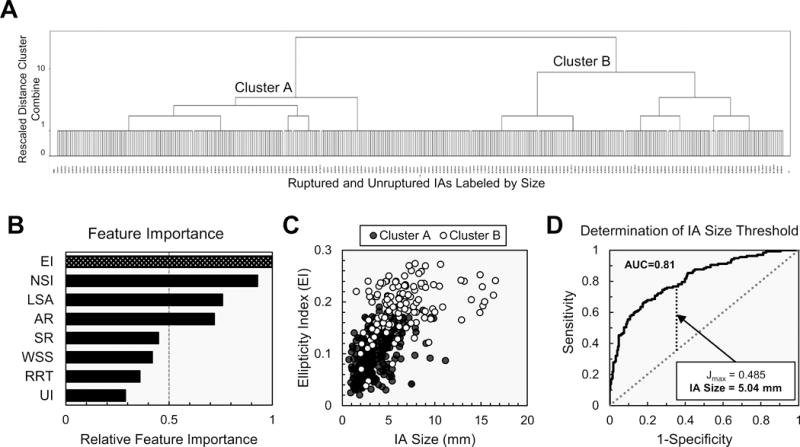
Methods: We analyzed morphological, hemodynamic, and clinical parameters of 413 retrospectively collected IAs (training cohort; 102 ruptured IAs). Hierarchal cluster analysis was performed to determine a size cutoff to dichotomize the IA population into small and large IAs. We applied multivariate logistic regression to build rupture discrimination models for small IAs, large IAs, and an aggregation of all IAs. We validated the ability of these 3 models to predict rupture status in a second, independently collected cohort of 129 IAs (testing cohort; 14 ruptured IAs).
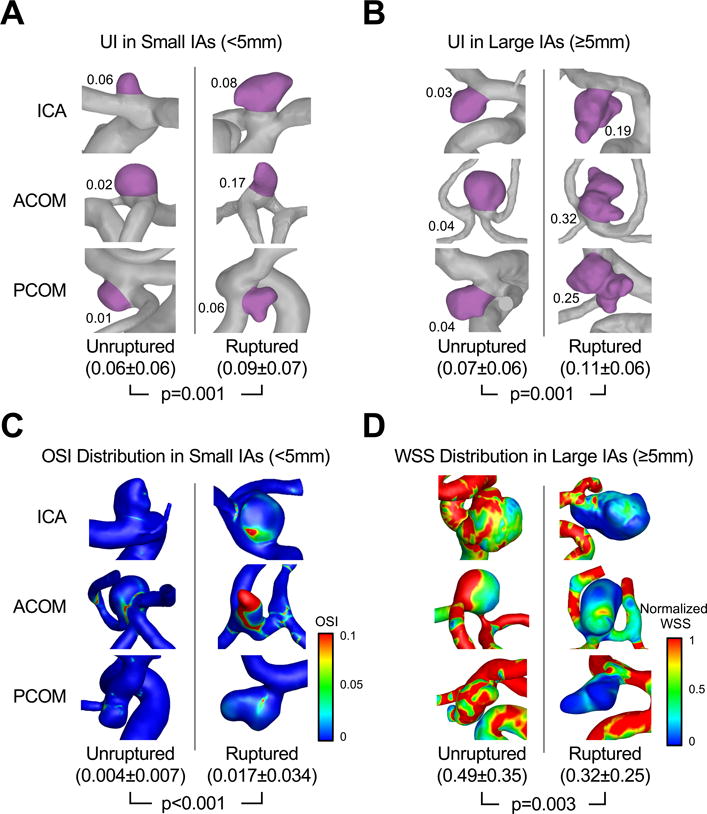
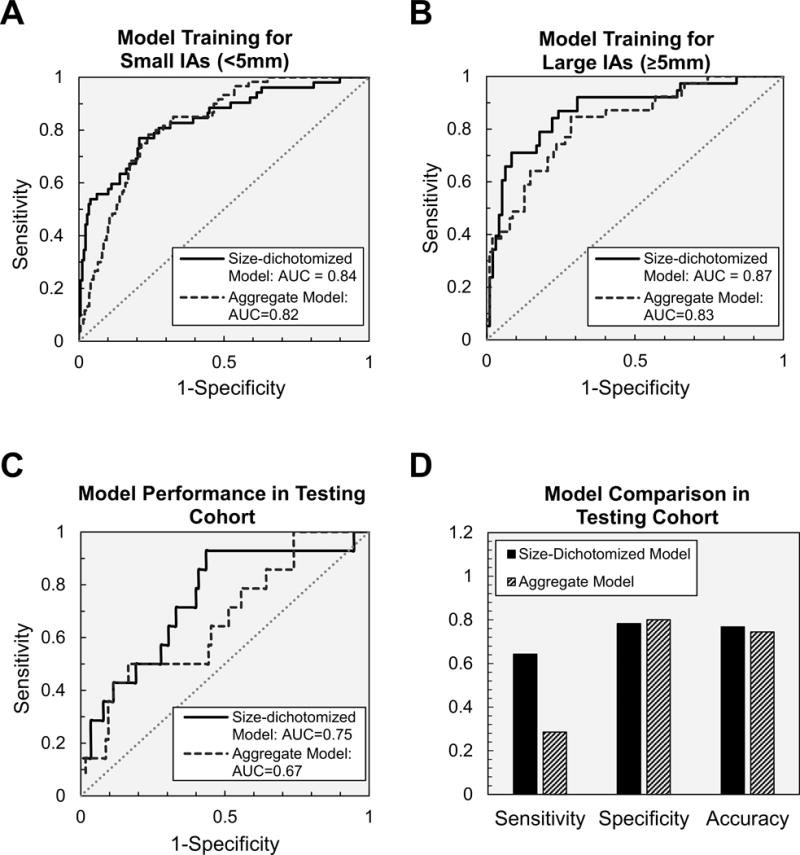
Results: Hierarchal cluster analysis in the training cohort confirmed that small and large IAs are best separated at 5 mm based on morphological and hemodynamic features (area under the curve=0.81). For small IAs (<5 mm), the resulting rupture discrimination model included undulation index, oscillatory shear index, previous subarachnoid hemorrhage, and absence of multiple IAs (area under the curve=0.84; 95% confidence interval, 0.78-0.88), whereas for large IAs (≥5 mm), the model included undulation index, low wall shear stress, previous subarachnoid hemorrhage, and IA location (area under the curve=0.87; 95% confidence interval, 0.82-0.93). The model for the aggregated training cohort retained all the parameters in the size-dichotomized models. Results in the testing cohort showed that the size-dichotomized rupture discrimination model had higher sensitivity (64% versus 29%) and accuracy (77% versus 74%), marginally higher area under the curve (0.75; 95% confidence interval, 0.61-0.88 versus 0.67; 95% confidence interval, 0.52-0.82), and similar specificity (78% versus 80%) compared with the aggregate-based model.
Conclusions: Small (<5 mm) and large (≥5 mm) IAs have different hemodynamic and clinical, but not morphological, rupture discriminants. Size-dichotomized rupture discrimination models performed better than the aggregate model.
Keywords: hemodynamics; intracranial aneurysm; machine learning; rupture.
© 2018 American Heart Association, Inc.
Conflict of interest statement
Varble:None
Tutino:Co-founder: Neurovascular Diagnostics, Inc.
Sonig:None
Siddiqui: Financial Interest: Apama Medical, Buffalo Technology Partners, Inc., Cardinal, Endostream Medical, Ltd., International Medical Distribution Partners, Medina Medical Systems, Neuro Technology Investors, StimMed, Valor Medical. Consultant: Amnis Therapeutics, Ltd., Cerebrotech Medical Systems, Inc., Cerenovus (Formerly Codman Neurovascular, Neuravi and Pulsar Vascular), CereVasc, LLC, Claret Medical, Inc., Corindus, Inc., GuidePoint Global Consulting, Integra (Formerly Codman Neurosurgery), Medtronic (Formerly Covidien), MicroVention, Neuravi (Now Cerenovus), Penumbra, Pulsar Vascular (Now Cerenovus), Rapid Medical, Rebound Therapeutics Corporation, Silk Road Medical, Stryker, The Stroke Project, Inc., Three Rivers Medical, Inc., Toshiba America Medical Systems, Inc., W.L. Gore & Associates. Advisory Board: Intersocietal Accreditation Commission. National Steering Committees: Codman & Shurtleff LARGE Trial, Covidien (Now Medtronic) SWIFT PRIME and SWIFT DIRECT Trials, MicroVention FRED Trial & CONFIDENCE Study, MUSC POSITIVE Trial, Penumbra 3D Separator Trial, COMPASS Trial, INVEST Trial, Neuravi ARISE II Trial Steering Committee
Davies:Research grant: NCATS KL2 grant. Speakers’ bureau: Penumbra; Honoraria: Neurotrauma Science, LLC
Figures
References
-
- Greving JP, Wermer MJ, Brown RD, Jr, Morita A, Juvela S, Yonekura M, et al. Development of the PHASES score for prediction of risk of rupture of intracranial aneurysms: a pooled analysis of six prospective cohort studies. Lancet Neurol. 2014;13:59–66. - PubMed
-
- Rinkel GJE, Djibuti M, Algra A, van Gijn J. Prevalence and risk of rupture of intracranial aneurysms: A systematic review. Stroke. 1998;29:251–256. - PubMed
-
- Wiebers DO. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet. 2003;362:103–110. - PubMed
-
- UCAS Japan Investigators. The Natural Course of Unruptured Cerebral Aneurysms in a Japanese Cohort. New Engl J Med. 2012;366:2474–2482. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
