

Role of Blood Lipids in the Development of Ischemic Stroke and its Subtypes: A Mendelian Randomization Study
- PMID: 29535274
- PMCID: PMC5895121
- DOI: 10.1161/STROKEAHA.117.019653
Role of Blood Lipids in the Development of Ischemic Stroke and its Subtypes: A Mendelian Randomization Study
Abstract
Background and purpose: Statin therapy is associated with a lower risk of ischemic stroke supporting a causal role of low-density lipoprotein (LDL) cholesterol. However, more evidence is needed to answer the question whether LDL cholesterol plays a causal role in ischemic stroke subtypes. In addition, it is unknown whether high-density lipoprotein cholesterol and triglycerides have a causal relationship to ischemic stroke and its subtypes. Our aim was to investigate the causal role of LDL cholesterol, high-density lipoprotein cholesterol, and triglycerides in ischemic stroke and its subtypes through Mendelian randomization (MR).
Methods: Summary data on 185 genome-wide lipids-associated single nucleotide polymorphisms were obtained from the Global Lipids Genetics Consortium and the Stroke Genetics Network for their association with ischemic stroke (n=16 851 cases and 32 473 controls) and its subtypes, including large artery atherosclerosis (n=2410), small artery occlusion (n=3186), and cardioembolic (n=3427) stroke. Inverse-variance-weighted MR was used to obtain the causal estimates. Inverse-variance-weighted multivariable MR, MR-Egger, and sensitivity exclusion of pleiotropic single nucleotide polymorphisms after Steiger filtering and MR-Pleiotropy Residual Sum and Outlier test were used to adjust for pleiotropic bias.
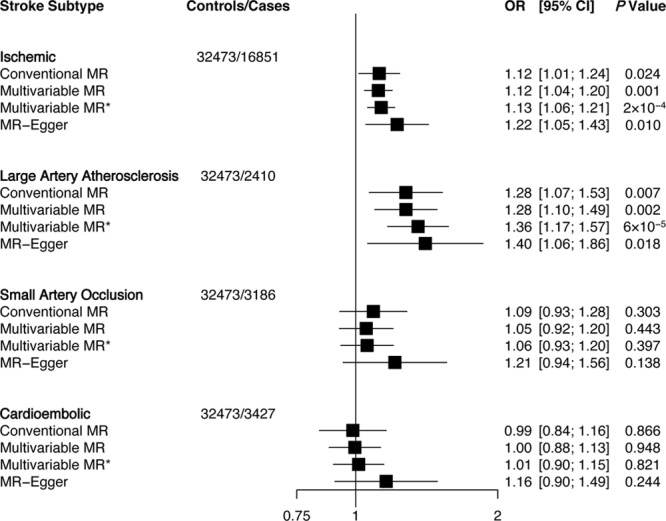
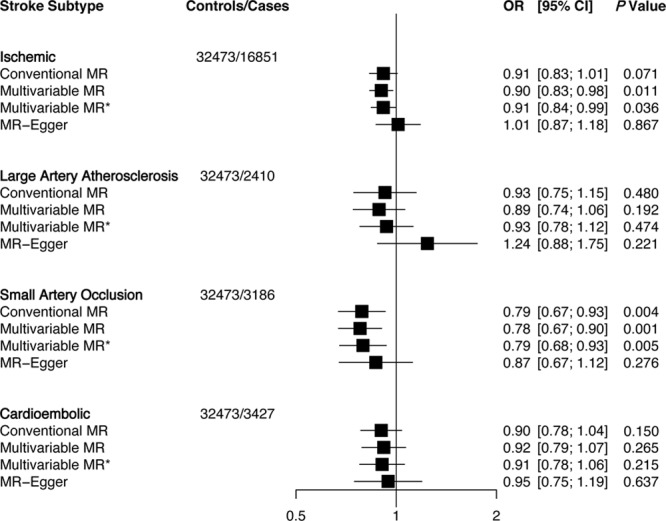
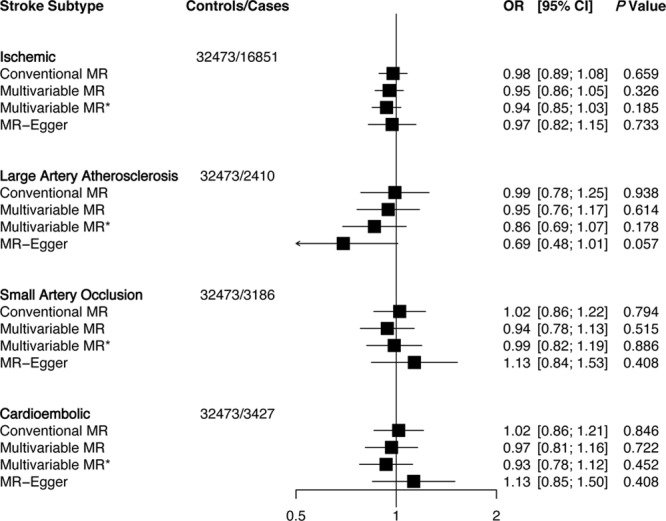
Results: A 1-SD genetically elevated LDL cholesterol was associated with an increased risk of ischemic stroke (odds ratio: 1.12; 95% confidence interval: 1.04-1.20) and large artery atherosclerosis stroke (odds ratio: 1.28; 95% confidence interval: 1.10-1.49) but not with small artery occlusion or cardioembolic stroke in multivariable MR. A 1-SD genetically elevated high-density lipoprotein cholesterol was associated with a decreased risk of small artery occlusion stroke (odds ratio: 0.79; 95% confidence interval: 0.67-0.90) in multivariable MR. MR-Egger indicated no pleiotropic bias, and results did not markedly change after sensitivity exclusion of pleiotropic single nucleotide polymorphisms. Genetically elevated triglycerides did not associate with ischemic stroke or its subtypes.
Conclusions: LDL cholesterol lowering is likely to prevent large artery atherosclerosis but may not prevent small artery occlusion nor cardioembolic strokes. High-density lipoprotein cholesterol elevation may lead to benefits in small artery disease prevention. Finally, triglyceride lowering may not yield benefits in ischemic stroke and its subtypes.
Keywords: cholesterol, HDL; cholesterol, LDL; polymorphism, single nucleotide; stroke; triglycerides.
© 2018 The Authors.
Figures
References
-
- Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, et al. Cholesterol Treatment Trialists’ (CTT) Collaboration. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376:1670–1681. doi: 10.1016/S0140-6736(10)61350-5. - PMC - PubMed
-
- Amarenco P, Bogousslavsky J, Callahan A, 3rd, Goldstein LB, Hennerici M, Rudolph AE, et al. Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) Investigators. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006;355:549–559. doi: 10.1056/NEJMoa061894. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
