

Benefit-risk profile of cytoreductive drugs along with antiplatelet and antithrombotic therapy after transient ischemic attack or ischemic stroke in myeloproliferative neoplasms
- PMID: 29535299
- PMCID: PMC5849668
- DOI: 10.1038/s41408-018-0048-9
Benefit-risk profile of cytoreductive drugs along with antiplatelet and antithrombotic therapy after transient ischemic attack or ischemic stroke in myeloproliferative neoplasms
Abstract
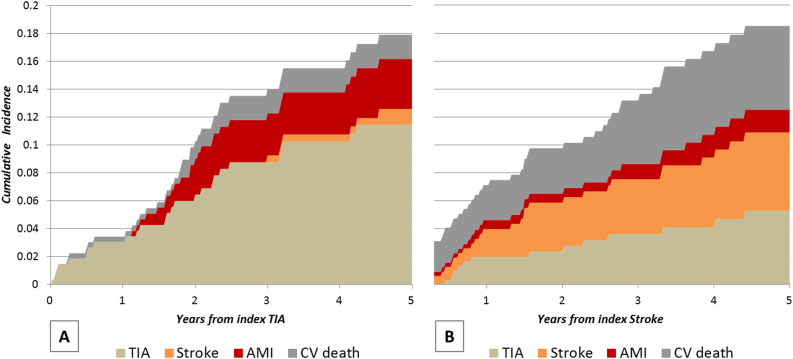
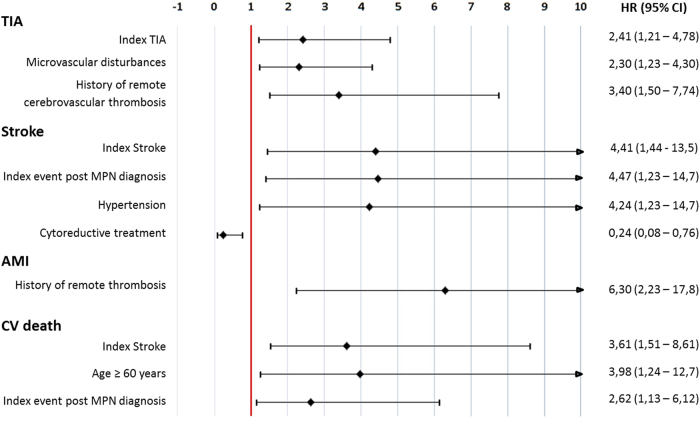
We analyzed 597 patients with myeloproliferative neoplasms (MPN) who presented transient ischemic attacks (TIA, n = 270) or ischemic stroke (IS, n = 327). Treatment included aspirin, oral anticoagulants, and cytoreductive drugs. The composite incidence of recurrent TIA and IS, acute myocardial infarction (AMI), and cardiovascular (CV) death was 4.21 and 19.2%, respectively at one and five years after the index event, an estimate unexpectedly lower than reported in the general population. Patients tended to replicate the first clinical manifestation (hazard ratio, HR: 2.41 and 4.41 for recurrent TIA and IS, respectively); additional factors for recurrent TIA were previous TIA (HR: 3.40) and microvascular disturbances (HR: 2.30); for recurrent IS arterial hypertension (HR: 4.24) and IS occurrence after MPN diagnosis (HR: 4.47). CV mortality was predicted by age over 60 years (HR: 3.98), an index IS (HR: 3.61), and the occurrence of index events after MPN diagnosis (HR: 2.62). Cytoreductive therapy was a strong protective factor (HR: 0.24). The rate of major bleeding was similar to the general population (0.90 per 100 patient-years). In conclusion, the long-term clinical outcome after TIA and IS in MPN appears even more favorable than in the general population, suggesting an advantageous benefit-risk profile of antithrombotic and cytoreductive treatment.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
