

The relationship between exercise capacity and different functional markers in pulmonary rehabilitation for COPD
- PMID: 29535512
- PMCID: PMC5836697
- DOI: 10.2147/COPD.S153525
The relationship between exercise capacity and different functional markers in pulmonary rehabilitation for COPD
Abstract
Rationale: The relationship of functional parameters such as lung mechanics, chest kinematics, metabolism and peripheral and respiratory muscle function with the level of exercise tolerance remains a controversial subject. While it has been previously shown that pulmonary rehabilitation is capable of improving exercise tolerance in patients afflicted by COPD, as expressed by values of 6-minute walking test (6MWT), the degree of contribution to this change by each of the aforementioned parameters remains unclear.
Aims: To investigate the correlation between changes in exercise capacity and other functional markers following pulmonary rehabilitation in COPD and to determine which parameters are more closely related to improvements of exercise tolerance.
Materials and methods: Three hundred and twenty-seven patients with COPD (with average, 95% CI for forced expiratory volume in the first second [FEV1]: 45% [25%-83%] predicted, age: 64 [48-80] years, and BMI: 27 [13.5-40.4] kg/m2) participated in this study. Thirty percent of the patients had pulmonary hypertension as comorbidity. Patients underwent a pulmonary rehabilitation program with 20-30 minutes sessions two to three times per day for 4 weeks. The program was composed of chest wall-stretching, controlled breathing exercises, and a personalized training schedule for cycling and treadmill use. Measurements of 6MWT, lung function, chest wall expansion, grip strength, maximal inspiratory pressure, and breath holding time were taken. The Body mass index, airflow Obstruction, Dyspnea and Exercise capacity (BODE-index), body mass index [BMI], FEV1, 6MWT, modified Medical Research Dyspnea Scale score, and an alternative scale score (for BMI, FEV1, 6MWT, and COPD Assessment Test) were calculated.
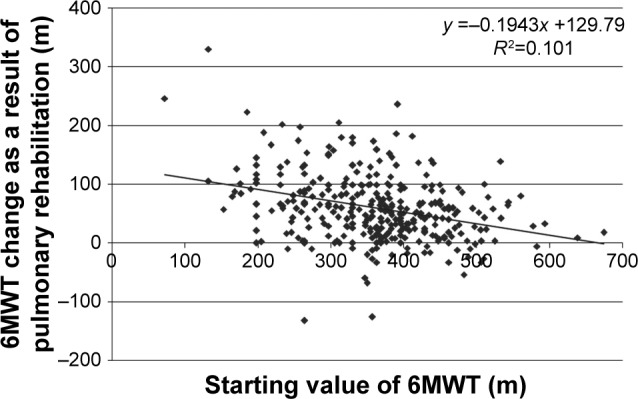
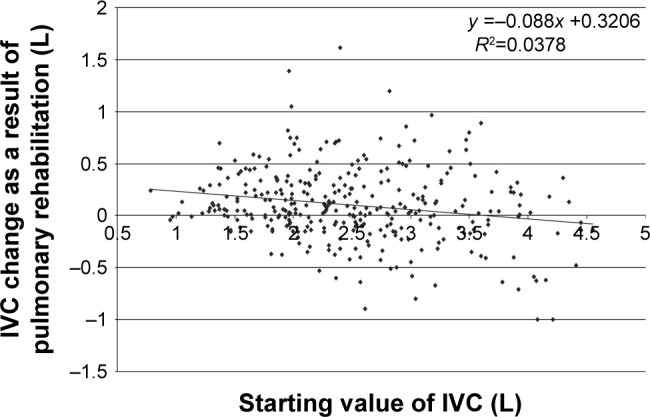
Results: Rehabilitation resulted in a generalized improvement in 6MWT among patients (average: 360 [95% CI: 178-543 m] vs average: 420 [95% CI: 238-601 m], p<0.05). Improvements in exercise tolerance were found to be most closely associated with changes in composite BODE-index (R2=-0.6), Alternative Scale (R2=-0.56), dyspnea score (modified Medical Research Dyspnea Scale R2=-0.54), and health status (COPD Assessment Test R2=-0.4, p<0.05). In addition, improvements in exercise tolerance were found to moderately correlate with improvements in inspiratory vital capacity (IVC, R2=0.34, p<0.05). Post-rehabilitation changes in IVC displayed a connection with grip strength (R2=0.6) and chest expansion (R2=0.48).
Conclusion: Enhancements in exercise tolerance had correlation with changes in IVC, BODE-index, and the new Alternative Scale. However, comprehensive assessment needs to include considerations of chest kinematics and peripheral and respiratory muscle function as well.
Keywords: breath holding time; exercise tolerance; health status; lung mechanics; respiratory and peripheral muscle function.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Cycle ergometer and inspiratory muscle training offer modest benefit compared with cycle ergometer alone: a comprehensive assessment in stable COPD patients.Int J Chron Obstruct Pulmon Dis. 2017 Sep 6;12:2655-2668. doi: 10.2147/COPD.S140093. eCollection 2017. Int J Chron Obstruct Pulmon Dis. 2017. PMID: 28919733 Free PMC article. Clinical Trial.
-
Effects of aerobic training combined with respiratory muscle stretching on the functional exercise capacity and thoracoabdominal kinematics in patients with COPD: a randomized and controlled trial.Int J Chron Obstruct Pulmon Dis. 2016 Oct 28;11:2691-2700. doi: 10.2147/COPD.S114548. eCollection 2016. Int J Chron Obstruct Pulmon Dis. 2016. PMID: 27822031 Free PMC article. Clinical Trial.
-
Inspiratory muscle training during pulmonary rehabilitation in chronic obstructive pulmonary disease: A randomized trial.Chron Respir Dis. 2015 Nov;12(4):305-12. doi: 10.1177/1479972315594625. Epub 2015 Jul 13. Chron Respir Dis. 2015. PMID: 26170421 Clinical Trial.
-
Optimal intensity and type of lower limb aerobic training for patients with chronic obstructive pulmonary disease: a systematic review and network meta-analysis of RCTs.Ther Adv Respir Dis. 2025 Jan-Dec;19:17534666251323190. doi: 10.1177/17534666251323190. Epub 2025 Mar 13. Ther Adv Respir Dis. 2025. PMID: 40083154 Free PMC article.
-
Effect of pulmonary rehabilitation for patients with long COVID-19: a systematic review and meta-analysis of randomized controlled trials.Ther Adv Respir Dis. 2025 Jan-Dec;19:17534666251323482. doi: 10.1177/17534666251323482. Epub 2025 Mar 13. Ther Adv Respir Dis. 2025. PMID: 40083165 Free PMC article.
Cited by
-
In vitro evidence of antioxidant and anti-inflammatory effects of a new nutraceutical formulation explains benefits in a clinical setting of COPD patients.Front Pharmacol. 2024 Aug 20;15:1439835. doi: 10.3389/fphar.2024.1439835. eCollection 2024. Front Pharmacol. 2024. PMID: 39228520 Free PMC article.
-
Impact of Exercise Capacity Upon Respiratory Functions, Perception of Dyspnea, and Quality of Life in Patients with Chronic Obstructive Pulmonary Disease.Int J Chron Obstruct Pulmon Dis. 2021 Jun 1;16:1529-1534. doi: 10.2147/COPD.S311221. eCollection 2021. Int J Chron Obstruct Pulmon Dis. 2021. PMID: 34103910 Free PMC article.
-
Motor and Respiratory Tele-Rehabilitation in Patients with Long COVID-19 after Hospital Discharge: An Interventional Study.Life (Basel). 2024 Jul 10;14(7):864. doi: 10.3390/life14070864. Life (Basel). 2024. PMID: 39063618 Free PMC article.
-
Respiratory muscle weakness and its association with exercise capacity in patients with chronic obstructive pulmonary disease.Clin Respir J. 2022 Feb;16(2):162-166. doi: 10.1111/crj.13449. Epub 2021 Oct 11. Clin Respir J. 2022. PMID: 34551459 Free PMC article.
-
Performance Score (T2D)-A New Perspective in the Assessment of Six-Minute Walking Tests in Pulmonary Rehabilitation.Diagnostics (Basel). 2022 Oct 3;12(10):2402. doi: 10.3390/diagnostics12102402. Diagnostics (Basel). 2022. PMID: 36292092 Free PMC article.
References
-
- Chaitow L, Breadly D, Gilbert C, Ley R. Multidisciplinary Approaches to Breathing Pattern Disorders. Amsterdam: Elsevier B.V.; 2013. The structure and function of breathing; pp. 1–41.
-
- Ambrosino N, Simonds A. The clinical management in extremely severe COPD. Respir Med. 2007;101(8):1613–1624. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
