

Relationship between the presence of bronchiectasis and acute exacerbation in Thai COPD patients
- PMID: 29535516
- PMCID: PMC5841335
- DOI: 10.2147/COPD.S139776
Relationship between the presence of bronchiectasis and acute exacerbation in Thai COPD patients
Abstract
Background: The prevalence rate of bronchiectasis in COPD is variable. Coexisting bronchiectasis and COPD may influence COPD severity and exacerbation.
Objective: We investigated whether bronchiectasis is associated with frequent or severe COPD exacerbation. Lower airway bacterial and mycobacterial infections are a possible mechanism for bronchiectasis.
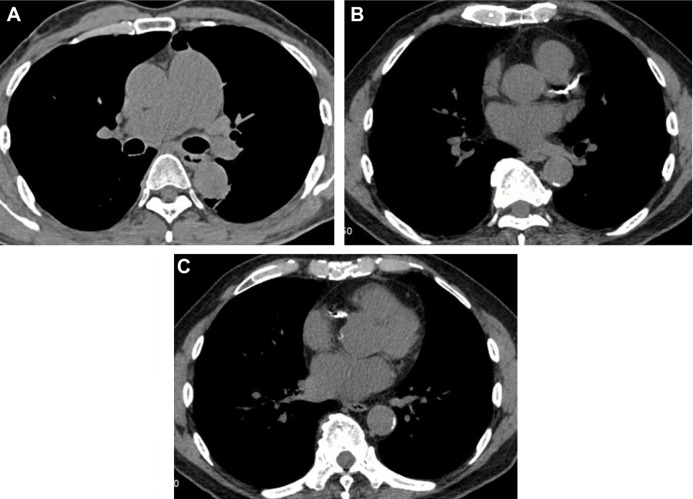
Materials and methods: A cross-sectional study was conducted in 2013-2014. COPD exacerbations and hospitalizations were reviewed. Spirometry and CT were performed. COPD symptoms were assessed by using the COPD assessment test (CAT) and modified Medical Research Council (mMRC) dyspnea scale. Sputum inductions were performed and specimens were sent for microbiology.
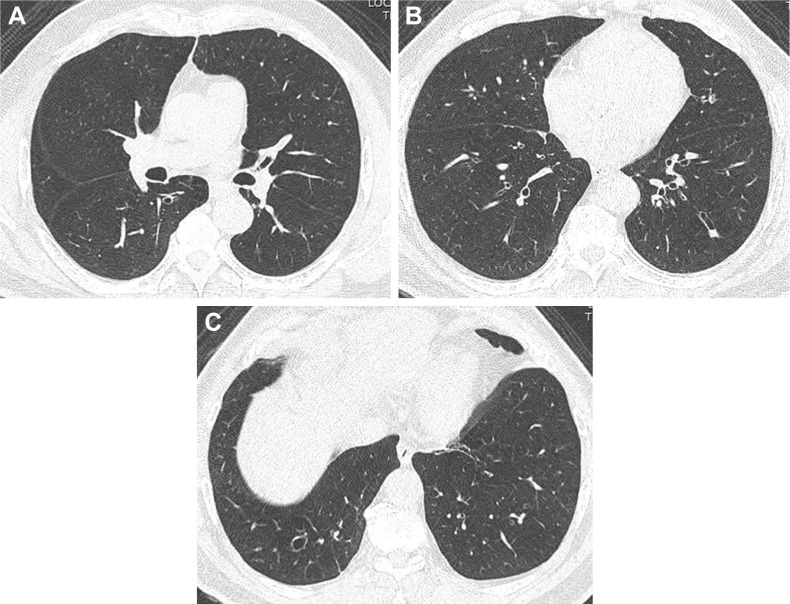
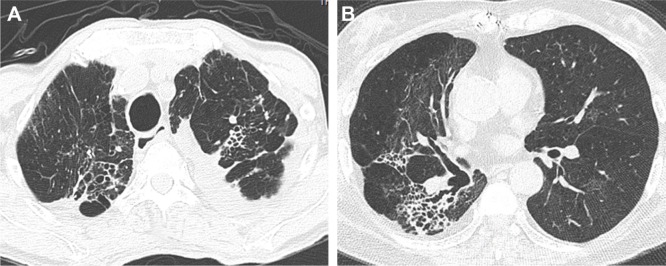
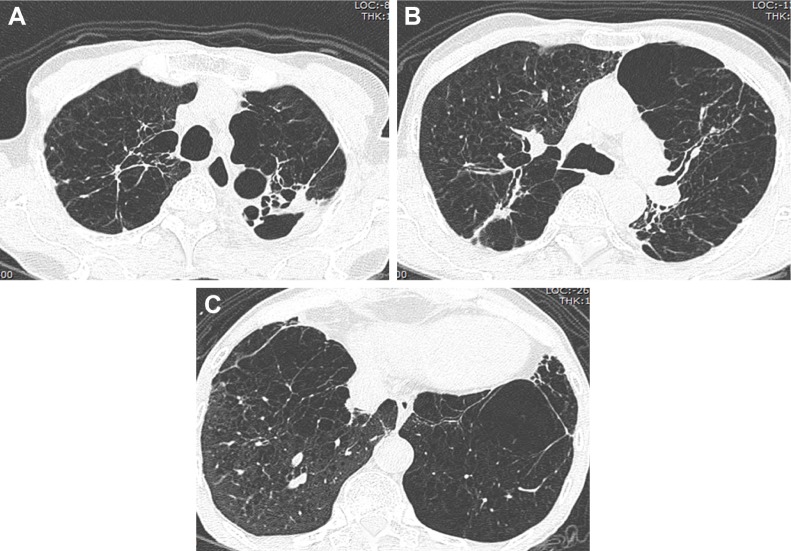
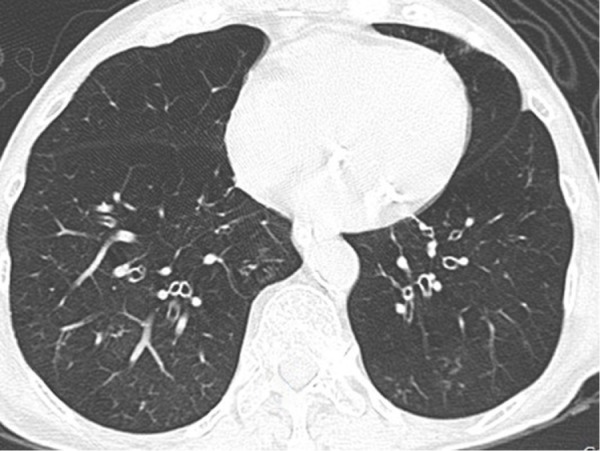
Results: We recruited 72 patients. Global Initiative for Chronic Obstructive Lung Disease (GOLD) A, B, C, and D, were noted in 20%, 27.1%, 14.3%, and 38.6% of the patients, respectively. Frequent exacerbations (≥2) and/or ≥1 hospitalization in the previous year were observed in 40.3% of patients. Median mMRC of COPD with frequent and non-frequent exacerbations was 1.0 (range 1-2) and 2.0 (range 1-3), (p=0.002), respectively. Median CAT of COPD with frequent and non-frequent exacerbations was 20.5 (3-37) and 11.0 (2-32), (p=0.004), respectively. CT-detected bronchiectasis was observed in 47.2% of patients. Median mMRC of COPD with and without bronchiectasis was 1.0 (0-4) and 1.0 (0-4) (p=0.22), respectively. Median CAT of COPD with and without bronchiectasis was 16.2 (95% CI: 12.9-19.6) and 13.0 (3-37), (p=0.49), respectively. The lower post-bronchodilator forced expiratory volume in 1 second (FEV1) of COPD with frequent exacerbations than those without was noted (p=0.007). The post-bronchodilator forced expiratory volume at 1 second percent in patients with and without bronchiectasis was not different (p=0.91). After adjusting for gender, severity of airflow obstruction, severity of COPD symptoms, the odds ratio for bronchiectasis with frequent and/or severe exacerbation was 4.99 (95% CI: 1.31-18.94), (p=0.018). Neither bacterial nor mycobacterial airway infection was associated with bronchiectasis or frequent exacerbation.
Conclusions: Bronchiectasis is common in Thai COPD. It was associated with frequent exacerbation or hospitalization. Mycobacterial tuberculosis in COPD patients with bronchiectasis was uncommon.
Keywords: COPD; bacteria; bronchiectasis; computed tomography; exacerbation; mycobacterium; prevalence; sputum.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures

Comment in
-
Impact of bronchiectasis on the frequency and severity of respiratory exacerbations in COPD.Int J Chron Obstruct Pulmon Dis. 2018 Jul 31;13:2335-2338. doi: 10.2147/COPD.S169760. eCollection 2018. Int J Chron Obstruct Pulmon Dis. 2018. PMID: 30104873 Free PMC article. No abstract available.
References
-
- Murray CJ, Lopez AD. Mortality by cause for eight regions of the world: Global Burden of Disease Study. Lancet. 1997;349(9061):1269–1276. - PubMed
-
- Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. - PubMed
-
- Global Strategy for the Diagnosis, Management and Prevention of COPD. 2014. [Accessed January 23, 2014]. Available from: www.goldcopd.com/guidelines-global-strategy-for-diagnosis-management.html.
-
- Rodriguez-Roisin R. Toward a consensus definition for COPD exacerbations. Chest. 2000;117(5 Suppl 2):398S–401S. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
