

Targeting DNA damage repair in small cell lung cancer and the biomarker landscape
- PMID: 29535912
- PMCID: PMC5835589
- DOI: 10.21037/tlcr.2018.02.03
Targeting DNA damage repair in small cell lung cancer and the biomarker landscape
Abstract
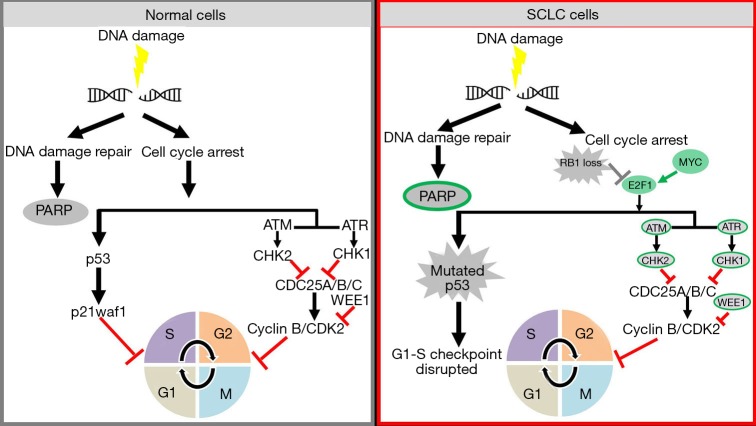
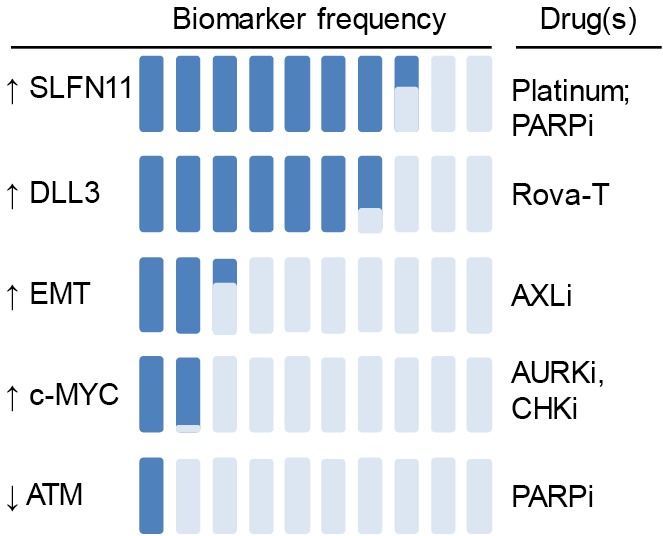
Small cell lung cancer (SCLC) is an aggressive malignancy that accounts for 14% of all lung cancer diagnoses. Despite decades of active research, treatment options for SCLC are limited and resistance to the few Food and Drug Administration (FDA) approved therapies develops rapidly. With no approved targeted agents to date, new therapeutic strategies are desperately needed. SCLC is characterized by high mutation burden, ubiquitous loss of TP53 and RB1, mutually exclusive amplification of MYC family members, thereby, high genomic instability. Studies in the past few years have demonstrated the potential of targeting the DNA damage response (DDR) pathway as a promising therapeutic strategy for SCLC. Inhibitors targeting DDR proteins have shown promise in preclinical models, and are under clinical investigation as single agents and in combination with cytotoxic therapies. Recent efforts to expand the therapeutic arsenal toward SCLC have focused in part on immune checkpoint inhibitors, such as agents targeting the receptor-ligand pair programmed cell death protein 1 (PD-1) and programmed death-ligand 1 (PD-L1). Clinical trials have confirmed activity of these agents in extensive stage (ES)-SCLC. However, while several patients had dramatic responses, overall response rates to immune checkpoint blockade (ICB) remain poor. As a result, there is an urgent need to develop rational combination therapies to enhance response rates to immunotherapy in SCLC. Identification of predictive biomarkers for patient stratification, identifying effective combinations to overcome adaptive resistance to DDR-targeted therapies and identifying strategies to enhance response to immunotherapy are areas of active investigation in SCLC.
Keywords: DNA damage response (DDR); biomarkers; immunotherapy; small cell lung cancer (SCLC).
Conflict of interest statement
Conflicts of Interest: LA Byers has served as an advisory board member and/or consultant to AstraZeneca, Medivation, and AbbVie.
Figures
References
-
- Nicholson AG, Chansky K, Crowley J, et al. The International Association for the Study of Lung Cancer Lung Cancer Staging Project: Proposals for the Revision of the Clinical and Pathologic Staging of Small Cell Lung Cancer in the Forthcoming Eighth Edition of the TNM Classification for Lung Cancer. J Thorac Oncol 2016;11:300-11. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous