Unilateral cleft lip repair: a comparison of treatment outcome with two surgical techniques using quantitative (anthropometry) assessment
- PMID: 29535963
- PMCID: PMC5845966
- DOI: 10.5125/jkaoms.2018.44.1.3
Unilateral cleft lip repair: a comparison of treatment outcome with two surgical techniques using quantitative (anthropometry) assessment
Abstract
Objectives: The unilateral cleft lip (UCL) repair technique has evolved extensively over the past century into its modern form and has been identified as an important determinant of treatment outcome. The aim of this study was to evaluate and compare treatment outcomes following repair of UCL using either the Tennison-Randall (triangular) technique or the Millard rotation-advancement technique.
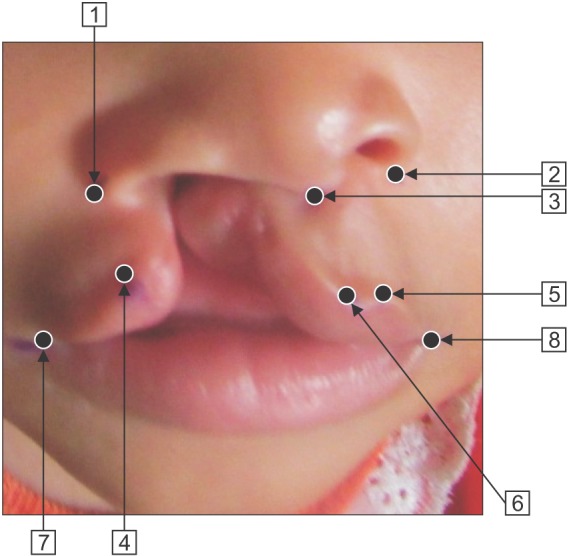
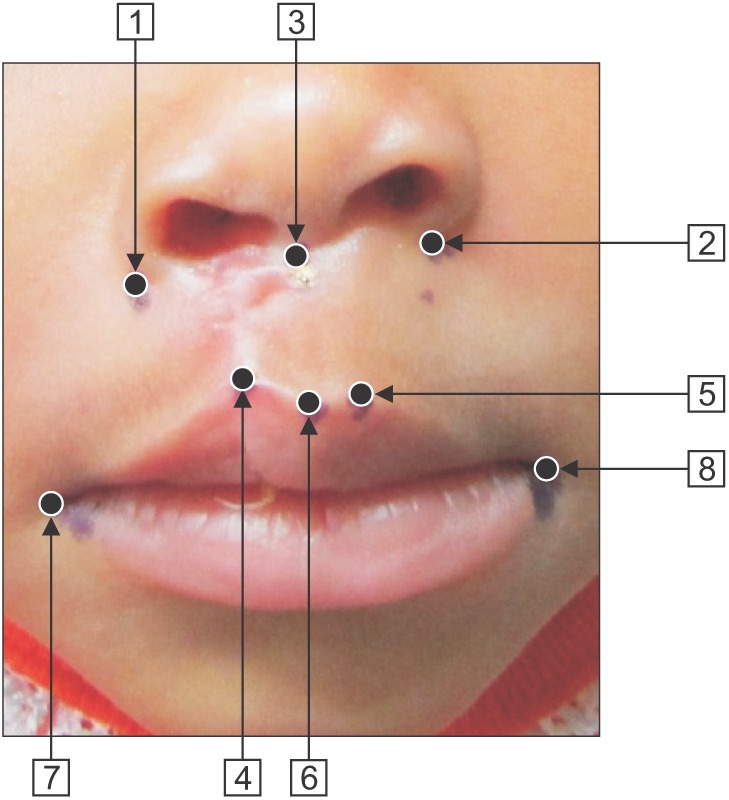
Materials and methods: This was a prospective randomized controlled study conducted at the Lagos University Teaching Hospital between January 2013 and July 2014. A total of 48 subjects with UCL presenting for primary surgery and who satisfied the inclusion criteria were recruited for the study. The subjects were randomly allocated into two surgical groups through balloting. Group A underwent cleft repair with the Tennison-Randall technique, while group B underwent cleft repair with the Millard rotation-advancement technique. Surgical outcome was assessed quantitatively according to anthropometric measurements, using a method described by Cutting and Dayan (2003).
Results: Our 48 enrolled subjects were evenly divided into the two surgery groups (n=24 for both group A and group B). Twenty-seven subjects were male (56.3%) and 21 were female (43.8%), making a sex ratio of 1.3:1. The Millard group showed a greater increase in postoperative horizontal length and vertical lip height and a greater reduction in nasal width and total nasal width. Meanwhile, the Tennison-Randall group showed better reduction of Cupid's-bow width and better philtral height.
Conclusion: We did not find any significant differences in the surgical outcomes from the two techniques. The expertise of the surgeon and individual patient preferences are the main factors to consider when selecting the technique for unilateral cleft repair.
Keywords: Anthropometry; Assessement; Cleft lip.
Conflict of interest statement
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Figures

Similar articles
-
Unilateral cleft lip: evaluation and comparison of treatment outcome with two surgical techniques based on qualitative (subject/guardian and professional) assessment.J Korean Assoc Oral Maxillofac Surg. 2019 Jun;45(3):141-151. doi: 10.5125/jkaoms.2019.45.3.141. Epub 2019 Jun 28. J Korean Assoc Oral Maxillofac Surg. 2019. PMID: 31334102 Free PMC article.
-
The Outcomes of Modified Millard Technique Versus Tennison-Randall Technique in Unilateral Cleft Lip Repair: A Comparative Trial.Afr J Paediatr Surg. 2024 Jan 1;21(1):12-17. doi: 10.4103/ajps.ajps_99_22. Epub 2023 Feb 14. Afr J Paediatr Surg. 2024. PMID: 38259014 Free PMC article. Clinical Trial.
-
Comparative Study between Modified Millard and White Roll Vermilion Flap Techniques in Unilateral Lip Repair: A Randomised Controlled Study.Afr J Paediatr Surg. 2024 Jan 1;21(1):18-27. doi: 10.4103/ajps.ajps_20_23. Epub 2024 Jan 20. Afr J Paediatr Surg. 2024. PMID: 38259015 Free PMC article. Clinical Trial.
-
Comparison of the rotation-advancement and philtral ridge techniques for unilateral cleft lip repair.Plast Reconstr Surg. 2014 Dec;134(6):1269-1278. doi: 10.1097/PRS.0000000000000723. Plast Reconstr Surg. 2014. PMID: 25255110
-
A comparative study of maxillary growth following rotation-advancement and triangular flap unilateral cleft lip repairs: an experimental study in rabbits.Ann Plast Surg. 2007 Apr;58(4):434-40. doi: 10.1097/01.sap.0000237645.58470.24. Ann Plast Surg. 2007. PMID: 17413888
Cited by
-
Multicenter Pattern of Cleft Surgeries and Factors Associated with Late Primary Cleft Surgery in Nigeria.Plast Reconstr Surg Glob Open. 2024 May 14;12(5):e5795. doi: 10.1097/GOX.0000000000005795. eCollection 2024 May. Plast Reconstr Surg Glob Open. 2024. PMID: 38746947 Free PMC article.
-
Effect of Cleft Types on Outcome of Unilateral Cleft Lip Repair.Ann Maxillofac Surg. 2020 Jul-Dec;10(2):297-303. doi: 10.4103/ams.ams_293_20. Epub 2020 Nov 10. Ann Maxillofac Surg. 2020. PMID: 33708571 Free PMC article.
-
Management of Orofacial Cleft in Nigeria - A Retrospective Study.Ann Maxillofac Surg. 2020 Jul-Dec;10(2):434-438. doi: 10.4103/ams.ams_104_20. Epub 2020 Dec 23. Ann Maxillofac Surg. 2020. PMID: 33708591 Free PMC article.
-
Treatment outcomes of two surgical techniques in secondary reconstruction of unilateral cleft lip and ala nasi utilizing anthropometry assessment: a randomized controlled trial.Maxillofac Plast Reconstr Surg. 2025 Jan 2;47(1):1. doi: 10.1186/s40902-024-00456-3. Maxillofac Plast Reconstr Surg. 2025. PMID: 39745524 Free PMC article.
-
Assessing Gender-Affirming Chest Surgery Outcomes: Does Gender Identity Alter Gaze?Aesthetic Plast Surg. 2021 Aug;45(4):1860-1868. doi: 10.1007/s00266-021-02378-1. Epub 2021 Jun 10. Aesthetic Plast Surg. 2021. PMID: 34114074
References
-
- Demke JC, Tatum SA. Analysis and evolution of rotation principles in unilateral cleft lip repair. J Plast Reconstr Aesthet Surg. 2011;64:313–318. - PubMed
-
- Arosarena OA. Cleft lip and palate. Otolaryngol Clin North Am. 2007;40:27–60. - PubMed
-
- Sykes JM. Management of the cleft lip deformity. Facial Plast Surg Clin North Am. 2001;9:37–50. - PubMed
-
- Kirschner RE, LaRossa D. Cleft lip and palate. Otolaryngol Clin North Am. 2000;33:1191–1215. - PubMed
-
- Nwoku AL. Experiences on the surgical repair of unoperated adult cleft patients in Nigeria. Niger Med J. 1976;4:417–421.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous