

Glioma imaging in Europe: A survey of 220 centres and recommendations for best clinical practice
- PMID: 29536240
- PMCID: PMC6028837
- DOI: 10.1007/s00330-018-5314-5
Glioma imaging in Europe: A survey of 220 centres and recommendations for best clinical practice
Abstract
Objectives: At a European Society of Neuroradiology (ESNR) Annual Meeting 2015 workshop, commonalities in practice, current controversies and technical hurdles in glioma MRI were discussed. We aimed to formulate guidance on MRI of glioma and determine its feasibility, by seeking information on glioma imaging practices from the European Neuroradiology community.
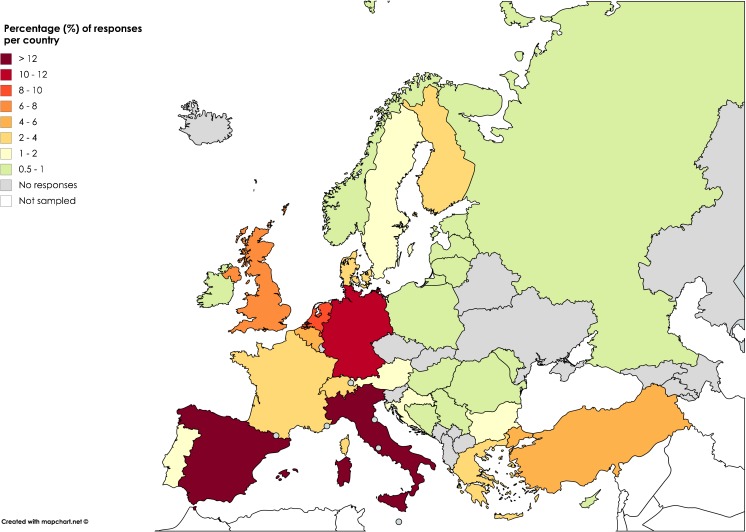
Methods: Invitations to a structured survey were emailed to ESNR members (n=1,662) and associates (n=6,400), European national radiologists' societies and distributed via social media.
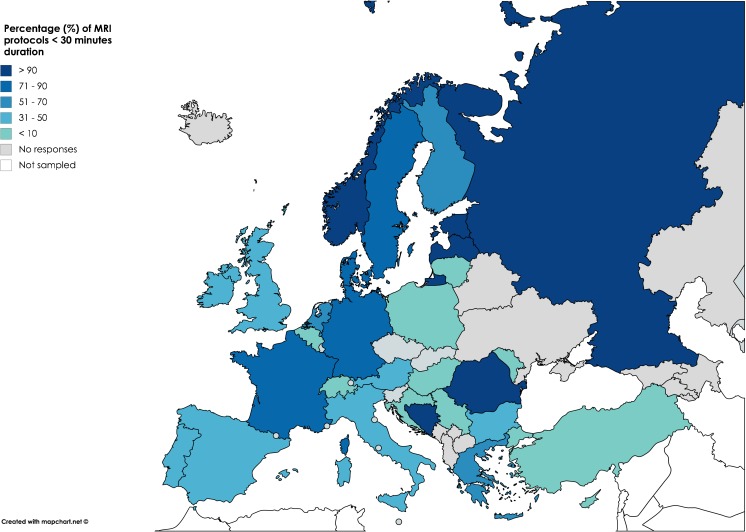
Results: Responses were received from 220 institutions (59% academic). Conventional imaging protocols generally include T2w, T2-FLAIR, DWI, and pre- and post-contrast T1w. Perfusion MRI is used widely (85.5%), while spectroscopy seems reserved for specific indications. Reasons for omitting advanced imaging modalities include lack of facility/software, time constraints and no requests. Early postoperative MRI is routinely carried out by 74% within 24-72 h, but only 17% report a percent measure of resection. For follow-up, most sites (60%) issue qualitative reports, while 27% report an assessment according to the RANO criteria. A minority of sites use a reporting template (23%).
Conclusion: Clinical best practice recommendations for glioma imaging assessment are proposed and the current role of advanced MRI modalities in routine use is addressed.
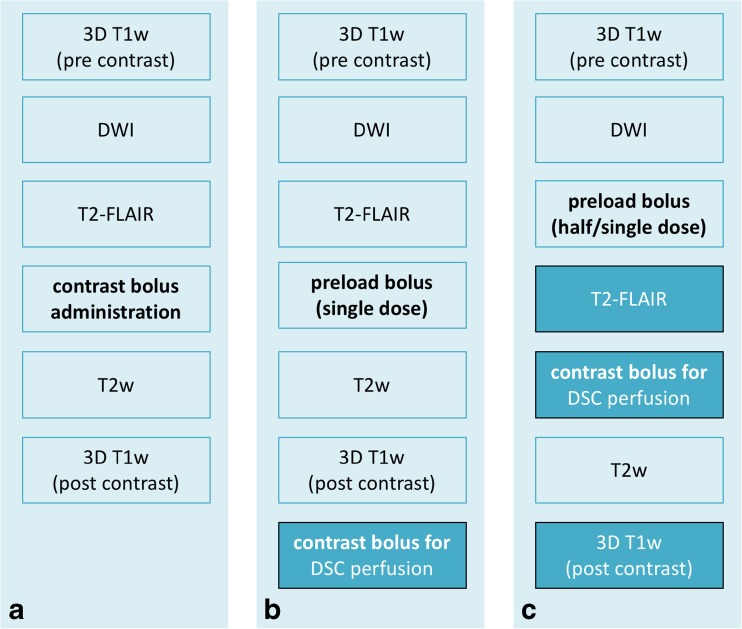
Key points: • We recommend the EORTC-NBTS protocol as the clinical standard glioma protocol. • Perfusion MRI is recommended for diagnosis and follow-up of glioma. • Use of advanced imaging could be promoted with increased education activities. • Most response assessment is currently performed qualitatively. • Reporting templates are not widely used, and could facilitate standardisation.
Keywords: Brain neoplasms; Glioma; Guideline; Magnetic resonance imaging; Surveys and questionnaires.
Conflict of interest statement
Guarantor
The scientific guarantor of this publication is M. Smits, MD PhD.
Conflict of interest
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Statistics and biometry
No complex statistical methods were necessary for this paper.
Informed consent
Written informed consent was not required for this study because no human subjects/patients were included in this study.
Ethical approval
Institutional Review Board approval was not required because no human subjects/patients were included in this study.
Methodology
• Survey and literature review.
Figures
References
-
- Patzig M, Burke M, Brückmann H, Fesl G. Comparison of 3D cube FLAIR with 2D FLAIR for multiple sclerosis imaging at 3 Tesla. Rofo. 2014;186:484–488. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
