

Time-dependent changes in extra-domain A-fibronectin concentration and relative amounts of fibronectin-fibrin complexes in plasma of patients with peripheral arterial disease after endovascular revascularisation
- PMID: 29536628
- PMCID: PMC7949812
- DOI: 10.1111/iwj.12909
Time-dependent changes in extra-domain A-fibronectin concentration and relative amounts of fibronectin-fibrin complexes in plasma of patients with peripheral arterial disease after endovascular revascularisation
Abstract
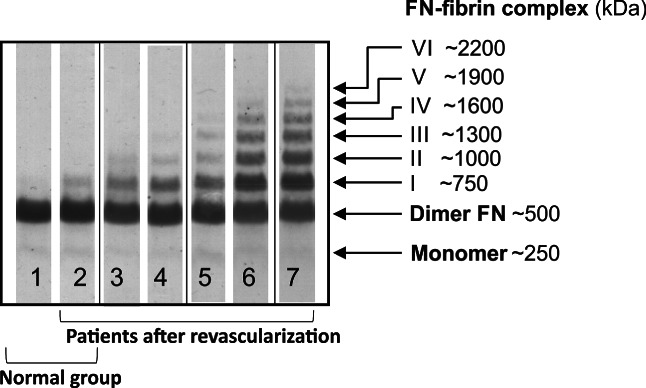
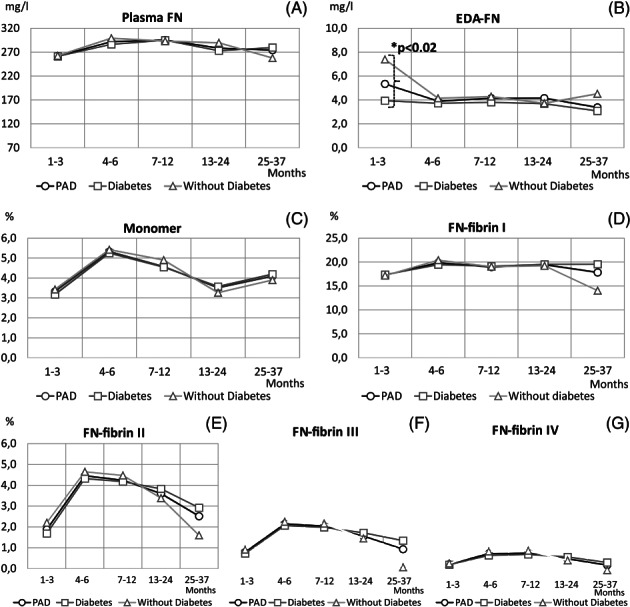
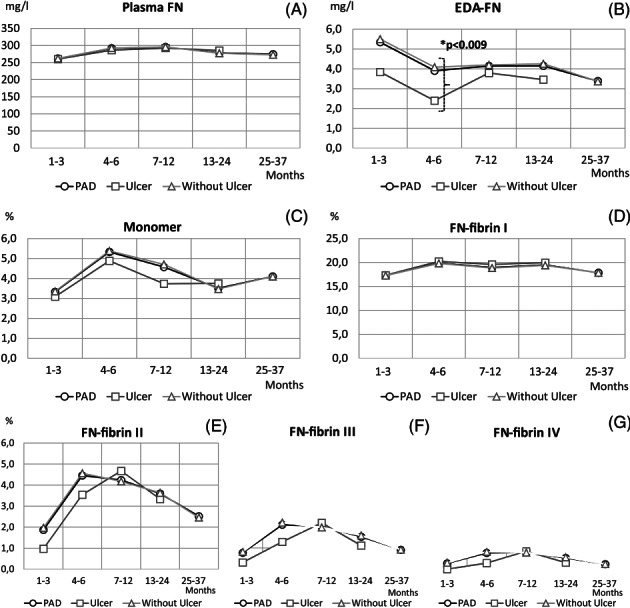
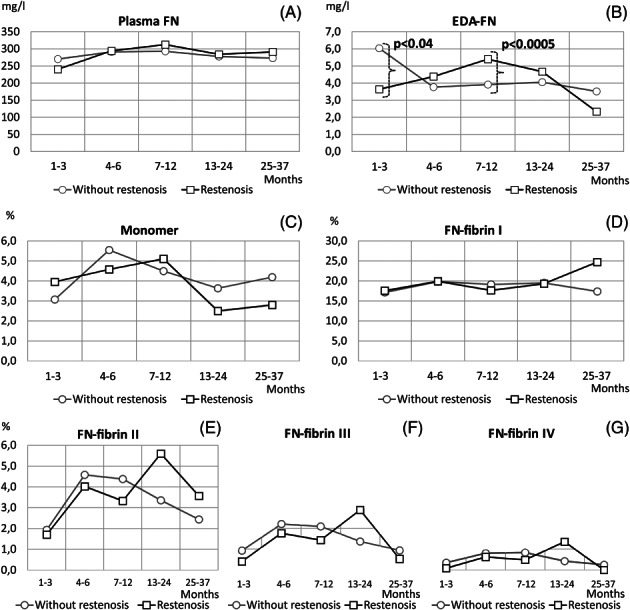
Fibronectin (FN) may be involved in time- and stage-dependent and inter-related controlled processes of inflammation, coagulation, and wound healing accompanying peripheral arterial disease (PAD). In the present study, FN and FN-containing extra-domain A (EDA-FN), macromolecular FN-fibrin complexes, and FN monomer were analysed in the plasma of 142 PAD patients, including 37 patients with restenosis, for 37 months after revascularisation. FN concentration increased significantly in the plasma of PAD patients within 7 to 12 months after revascularisation, whereas the high concentration of EDA-FN was maintained up to 24 months, significantly higher in the group 7 to 12 months after revascularisation with recurrence of stenosis and lower in the PAD groups 1 to 3 months and 4 to 6 months after revascularisation with comorbid diabetes and ulceration, respectively. The relative amounts of FN-fibrin complexes up to 1600 kDa and FN monomer were significantly higher, within intervals of 4 to 24 months and 4 to 6 months after revascularisation, respectively. Moreover, the relative amounts of 750 to 1600 kDa FN-fibrin complexes within 13 to 24 months after revascularisation were higher in comparison with those in the group without restenosis. In conclusion, high levels of EDA-FN and FN-fibrin complexes could have potential diagnostic value in the management of PAD patients after revascularisation, predicting restenosis risk.
Keywords: EDA-fibronectin; FN-fibrin complexes; fibronectin; peripheral arterial disease; restenosis.
© 2018 Medicalhelplines.com Inc and John Wiley & Sons Ltd.
Conflict of interest statement
The authors have no competing interests to declare.
Figures
Similar articles
-
Analysis of Soluble Molecular Fibronectin-Fibrin Complexes and EDA-Fibronectin Concentration in Plasma of Patients with Atherosclerosis.Inflammation. 2016 Jun;39(3):1059-68. doi: 10.1007/s10753-016-0336-0. Inflammation. 2016. PMID: 27022744 Free PMC article.
-
Occurrence of fibronectin-fibrin complexes in plasma of patients with multimorbidity due to the inflamm-aging phenomenon.Exp Gerontol. 2016 May;77:19-28. doi: 10.1016/j.exger.2016.02.006. Epub 2016 Feb 13. Exp Gerontol. 2016. PMID: 26883337
-
Identification of soluble supramolecular FN-fibrin complexes in human plasma.J Immunoassay Immunochem. 2014;35(4):412-27. doi: 10.1080/15321819.2014.885448. J Immunoassay Immunochem. 2014. PMID: 24547768
-
Fibronectin and its soluble EDA-FN isoform as biomarkers for inflammation and sepsis.Adv Clin Exp Med. 2019 Nov;28(11):1561-1567. doi: 10.17219/acem/104531. Adv Clin Exp Med. 2019. PMID: 31596557 Review.
-
Effectiveness of revascularisation of the ulcerated foot in patients with diabetes and peripheral artery disease: A systematic review.Diabetes Metab Res Rev. 2020 Mar;36 Suppl 1:e3279. doi: 10.1002/dmrr.3279. Diabetes Metab Res Rev. 2020. PMID: 32176439
Cited by
-
Role of Infection and Immunity in Bovine Perinatal Mortality: Part 2. Fetomaternal Response to Infection and Novel Diagnostic Perspectives.Animals (Basel). 2021 Jul 15;11(7):2102. doi: 10.3390/ani11072102. Animals (Basel). 2021. PMID: 34359230 Free PMC article. Review.
-
Fibronectin Molecular Status in Plasma of Women with Endometriosis and Fertility Disorders.Int J Mol Sci. 2021 Oct 22;22(21):11410. doi: 10.3390/ijms222111410. Int J Mol Sci. 2021. PMID: 34768846 Free PMC article.
-
Cellular fibronectin promotes deep vein thrombosis in diet-induced obese mice.J Thromb Haemost. 2021 Mar;19(3):814-821. doi: 10.1111/jth.15206. Epub 2020 Dec 27. J Thromb Haemost. 2021. PMID: 33300307 Free PMC article.
-
Changes of plasma fibronectin and fibronectin-fibrin complexes in dams of stillborn dairy calves.Ir Vet J. 2020 Aug 9;73:17. doi: 10.1186/s13620-020-00171-1. eCollection 2020. Ir Vet J. 2020. PMID: 32788999 Free PMC article.
References
-
- Jones WS, Schmit KM, Vemulapalli S, et al. Treatment Strategies for Patients With Peripheral Artery Disease. Vol 118. Rockville, MD: AHRQ Comparative Effectiveness Review; 2013. Report No.: 13‐EHC090‐EF.
-
- Hiatt WR, Goldstone J, Smith SC Jr, et al. Atherosclerotic peripheral vascular disease symposium II: nomenclature for vascular diseases. Circulation. 2008;118:2826‐2829. - PubMed
-
- Dangas GD, Claessen BE, Caixeta A, Sanidas EA, Mintz GS, Mehran R. In‐stent restenosis in the drug‐eluting stent era. J Am Coll Cardiol. 2010;56(10):1897‐1907. - PubMed
-
- Belay T. Endothelial repair and regeneration following intimal injury. J Cardiovasc Transl Res. 2016;9(2):91‐101. - PubMed
-
- Otsuka F, Byrne RA, Yahagi K, et al. Neoatherosclerosis: overview of histopathologic findings and implications for intravascular imaging assessment. Eur Heart J. 2015;36(32):2147‐2159. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
