

Risk and protective factors for obstetric anal sphincter injuries: A retrospective nationwide study
- PMID: 29537100
- PMCID: PMC6282595
- DOI: 10.1111/birt.12346
Risk and protective factors for obstetric anal sphincter injuries: A retrospective nationwide study
Abstract
Background: In view of the reported increase in obstetric anal sphincter injuries, the objective of this study was to evaluate the incidence of such injuries over time and the associated risk and protective factors.
Methods: This was a retrospective cohort study from a national database of 168 137 primiparous women with term, singleton, cephalic, vaginal delivery between 2008 and 2014. The main outcome measure was obstetric anal sphincter injury. A multivariate regression model was used to identify risk and protective factors.
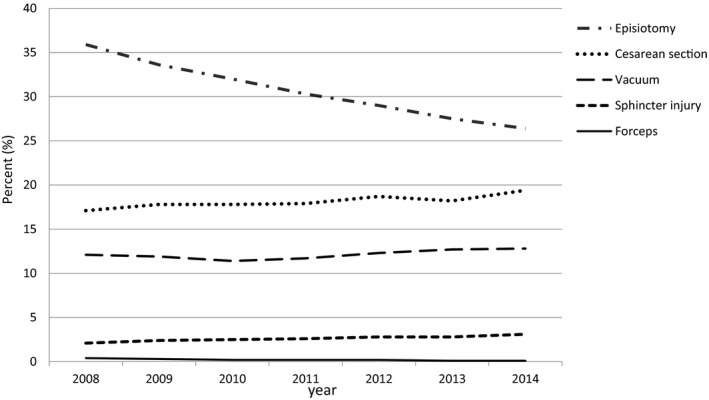
Results: Age >19 years, birthweight >4000 g, and operative vaginal delivery were independent risk factors for obstetric anal sphincter injuries. Mediolateral episiotomy increased the risk for obstetric anal sphincter injuries in spontaneous vaginal birth (number needed to harm 333), whereas it was protective in vacuum delivery (number needed to treat 50). From 2008 to 2014, there was an increase in the rate of obstetric anal sphincter injuries (2.1% vs 3.1%, P < .01), vacuum deliveries (12.1% vs 12.8%, P < .01), and cesarean delivery after labor (17.1% vs 19.4%, P < .01), while forceps deliveries (0.4% vs 0.1%, P < .01) and episiotomy rate decreased (35.9% vs 26.4%, P < .01).
Conclusions: Episiotomy may be a risk or protective factor depending on the type of episiotomy and the clinical setting in which it is used. Our study supports a restrictive use of mediolateral episiotomy in spontaneous vaginal deliveries. In vacuum deliveries mediolateral episiotomy may help prevent obstetric anal sphincter injuries.
Keywords: episiotomy; obstetric anal sphincter injury; risk factors.
© 2018 the Authors. Birth published by Wiley Periodicals, Inc.
Figures
Similar articles
-
Mediolateral episiotomy and obstetric anal sphincter injuries in nullipara: a propensity score matching study.BMC Pregnancy Childbirth. 2025 Jan 27;25(1):76. doi: 10.1186/s12884-025-07184-0. BMC Pregnancy Childbirth. 2025. PMID: 39871193 Free PMC article.
-
Episiotomy use among vaginal deliveries and the association with anal sphincter injury: a population-based retrospective cohort study.CMAJ. 2019 Oct 21;191(42):E1149-E1158. doi: 10.1503/cmaj.190366. CMAJ. 2019. PMID: 31636163 Free PMC article.
-
Mediolateral episiotomy reduces the risk for anal sphincter injury during operative vaginal delivery.BJOG. 2008 Jan;115(1):104-8. doi: 10.1111/j.1471-0528.2007.01554.x. Epub 2007 Nov 12. BJOG. 2008. PMID: 17999693
-
The prevention of perineal trauma during vaginal birth.Am J Obstet Gynecol. 2024 Mar;230(3S):S991-S1004. doi: 10.1016/j.ajog.2022.06.021. Epub 2023 Aug 11. Am J Obstet Gynecol. 2024. PMID: 37635056 Review.
-
Obstetric anal sphincter injuries - review of our date between 2015-2017.Ceska Gynekol. 2019 Winter;84(1):18-22. Ceska Gynekol. 2019. PMID: 31213053 Review. English.
Cited by
-
Delivery Mode after Ileal Pouch-Anal Anastomosis among Pregnant Women with Ulcerative Colitis.J Anus Rectum Colon. 2021 Oct 28;5(4):419-425. doi: 10.23922/jarc.2021-022. eCollection 2021. J Anus Rectum Colon. 2021. PMID: 34746507 Free PMC article.
-
Impact of a quality improvement project to reduce the rate of obstetric anal sphincter injury: a multicentre study with a stepped-wedge design.BJOG. 2021 Feb;128(3):584-592. doi: 10.1111/1471-0528.16396. Epub 2020 Aug 9. BJOG. 2021. PMID: 33426798 Free PMC article.
-
Can We Predict Feto-Maternal Adverse Outcomes of Vacuum Extraction?Geburtshilfe Frauenheilkd. 2022 Sep 7;82(11):1274-1282. doi: 10.1055/a-1904-6025. eCollection 2022 Nov. Geburtshilfe Frauenheilkd. 2022. PMID: 36339635 Free PMC article.
-
Randomized, Double-Blind, Placebo-Controlled Trial on the Efficacy of Hyaluronidase in Preventing Perineal Trauma in Nulliparous Women.Yonsei Med J. 2020 Jan;61(1):79-84. doi: 10.3349/ymj.2020.61.1.79. Yonsei Med J. 2020. PMID: 31887803 Free PMC article. Clinical Trial.
-
Obstetric anal sphincter injuries-Maternal, fetal and sociodemographic risk factors: A retrospective register-based study.Acta Obstet Gynecol Scand. 2022 Nov;101(11):1262-1268. doi: 10.1111/aogs.14425. Epub 2022 Aug 3. Acta Obstet Gynecol Scand. 2022. PMID: 35920107 Free PMC article.
References
-
- Sultan AH. Obstetric perineal injury and anal incontinence. Clin Risk. 1999;5:193‐196.
-
- Vale de Castro Monteiro M, Pereira GM, Aguiar RA, Azevedo RL, Correia‐Junior MD, Reis ZS. Risk factors for severe obstetric perineal lacerations. Int Urogynecol J. 2016;27:61‐67. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
