

Impact of the Four-Hour Rule in Western Australian hospitals: Trend analysis of a large record linkage study 2002-2013
- PMID: 29538401
- PMCID: PMC5851625
- DOI: 10.1371/journal.pone.0193902
Impact of the Four-Hour Rule in Western Australian hospitals: Trend analysis of a large record linkage study 2002-2013
Abstract
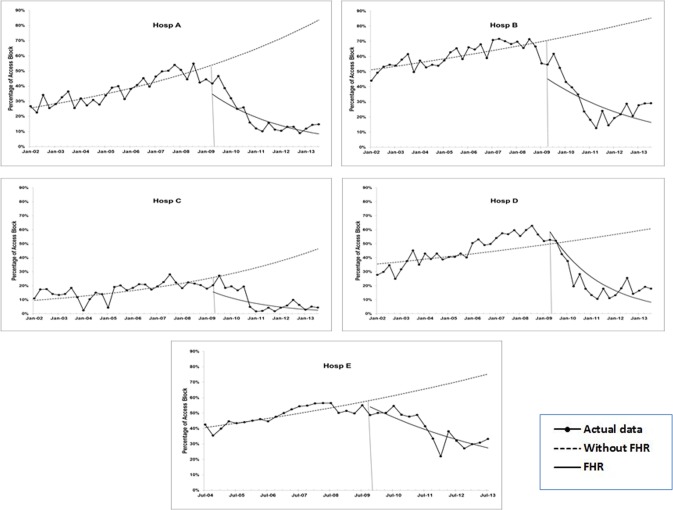
Background: In 2009, the Western Australian (WA) Government introduced the Four-Hour Rule (FHR) program. The policy stated that most patients presenting to Emergency Departments (EDs) were to be seen and either admitted, transferred, or discharged within 4 hours. This study utilised de-identified data from five participating hospitals, before and after FHR implementation, to assess the impact of the FHR on several areas of ED functioning.
Methods: A state (WA) population-based intervention study design, using longitudinal data obtained from administrative health databases via record linkage methodology, and interrupted time series analysis technique.
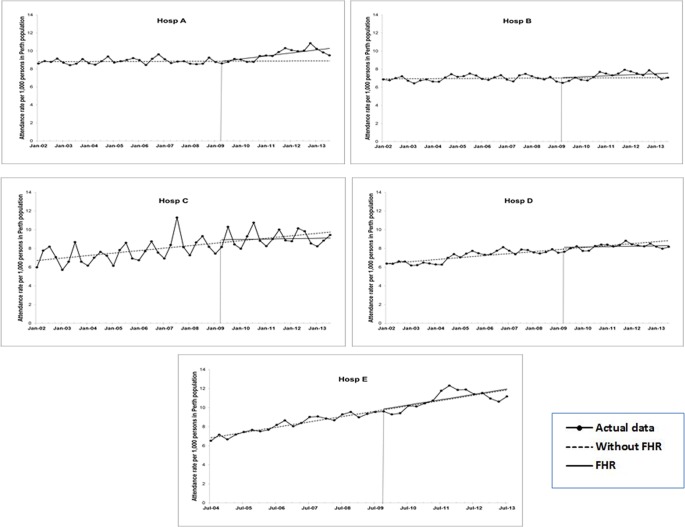
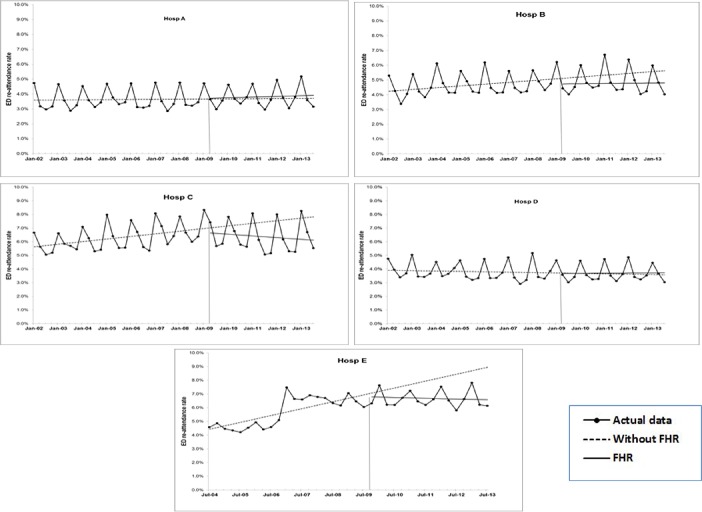
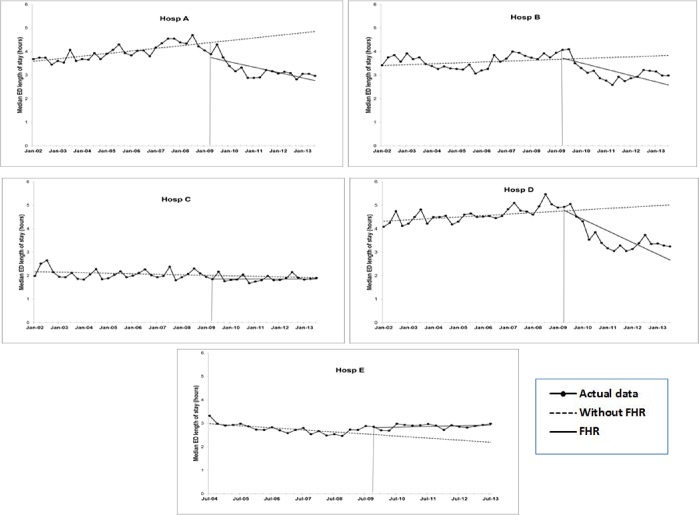
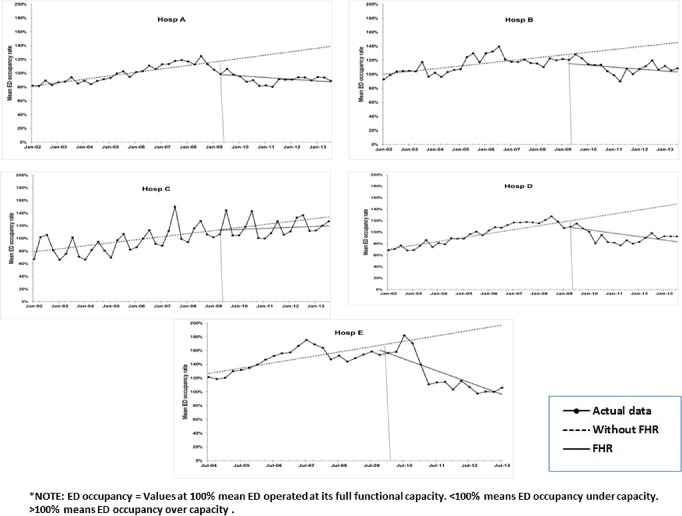
Findings: There were 3,214,802 ED presentations, corresponding to 1,203,513 ED patients. After the FHR implementation, access block for patients admitted through ED for all five sites showed a significant reduction of up to 13.2% (Rate Ratio 0.868, 95%CI 0.814, 0.925) per quarter. Rate of ED attendances for most hospitals continued to rise throughout the entire study period and were unaffected by the FHR, except for one hospital. Pattern of change in ED re-attendance rate post-FHR was similar to pre-FHR, but the trend reduced for two hospitals. ED occupancy was reduced by 6.2% per quarter post-FHR for the most 'crowded' ED. ED length of stay and ED efficiency improved in four hospitals and deteriorated in one hospital. Time to being seen by ED clinician and Did-Not-Wait rate improved for some hospitals. Admission rates in post-FHR increased, by up to 1% per quarter, for two hospitals where the pre-FHR trend was decreasing.
Conclusions: The FHR had a consistent effect on 'flow' measures: significantly reducing ED overcrowding and access block and enhancing ED efficiency. Time-based outcome measures mostly improved with the FHR. There is some evidence of increased ED attendance, but no evidence of increased ED re-attendance. Effects on patient disposition status were mixed. Overall, this reflects the value of investing resources into the ED/hospital system to improve efficiency and patient experience. Further research is required to illuminate the exact mechanisms of the effects of FHR on the ED and hospital functioning across Australia.
Conflict of interest statement
Figures
Similar articles
-
Impact of the four-hour National Emergency Access Target on 30 day mortality, access block and chronic emergency department overcrowding in Australian emergency departments.Emerg Med Australas. 2019 Feb;31(1):58-66. doi: 10.1111/1742-6723.13151. Epub 2018 Jul 30. Emerg Med Australas. 2019. PMID: 30062847
-
Impact of the Four-Hour Rule policy on emergency medical services delays in Australian EDs: a longitudinal cohort study.Emerg Med J. 2020 Dec;37(12):793-800. doi: 10.1136/emermed-2019-208958. Epub 2020 Jul 15. Emerg Med J. 2020. PMID: 32669320
-
The association between hospital overcrowding and mortality among patients admitted via Western Australian emergency departments.Med J Aust. 2006 Mar 6;184(5):208-12. doi: 10.5694/j.1326-5377.2006.tb00416.x. Med J Aust. 2006. PMID: 16515429
-
The role of full capacity protocols on mitigating overcrowding in EDs.Am J Emerg Med. 2012 Mar;30(3):412-20. doi: 10.1016/j.ajem.2010.12.035. Epub 2011 Mar 1. Am J Emerg Med. 2012. PMID: 21367554 Review.
-
Evaluating mental health decision units in acute care pathways (DECISION): a quasi-experimental, qualitative and health economic evaluation.Health Soc Care Deliv Res. 2023 Dec;11(25):1-221. doi: 10.3310/PBSM2274. Health Soc Care Deliv Res. 2023. PMID: 38149657
Cited by
-
Impact of the 24-hour time target policy for emergency departments in South Korea: a mixed method study in a single medical center.BMC Health Serv Res. 2022 Dec 12;22(1):1510. doi: 10.1186/s12913-022-08861-y. BMC Health Serv Res. 2022. PMID: 36510204 Free PMC article.
-
"Time is of the essence": relationship between hospital staff perceptions of time, safety attitudes and staff wellbeing.BMC Health Serv Res. 2021 Nov 20;21(1):1256. doi: 10.1186/s12913-021-07275-6. BMC Health Serv Res. 2021. PMID: 34801004 Free PMC article.
-
Factors Affecting Length of Stays in the Emergency Department of a Teaching Hospital: A Retrospective Study From Najran, Saudi Arabia.Cureus. 2024 Jul 16;16(7):e64684. doi: 10.7759/cureus.64684. eCollection 2024 Jul. Cureus. 2024. PMID: 39149637 Free PMC article.
-
The goldilocks effect: the rhythms and pace of hospital life.BMC Health Serv Res. 2018 Jul 6;18(1):529. doi: 10.1186/s12913-018-3350-0. BMC Health Serv Res. 2018. PMID: 29980227 Free PMC article.
-
A multivariable analysis to predict variations in hospital mortality using systems-based factors of healthcare delivery to inform improvements to healthcare design within the English NHS.PLoS One. 2024 Jul 5;19(7):e0303932. doi: 10.1371/journal.pone.0303932. eCollection 2024. PLoS One. 2024. PMID: 38968314 Free PMC article.
References
-
- Forero R, McCarthy S, Hillman K. Access block and emergency department overcrowding. Critical Care. 2011;15(2):216–22. doi: 10.1186/cc9998 - DOI - PMC - PubMed
-
- Gillman L, Fatovich D, Jacobs I. Mortality of interhospital transfers originating from an emergency department in Perth, Western Australia. Australasian Emergency Nursing Journal. 2013;16(4):144–51. doi: 10.1016/j.aenj.2013.07.001 . - DOI - PubMed
-
- Fatovich DM, Nagree Y, Sprivulis P. Access block causes emergency department overcrowding and ambulance diversion in Perth, Western Australia.[Erratum appears in Emerg Med J. 2005 Jul;22(7):532]. Emergency Medicine Journal. 2005;22(5):351–4. doi: 10.1136/emj.2004.018002 ; PubMed Central PMCID: PMCPMC1726785. - DOI - PMC - PubMed
-
- Sprivulis PC, Da Silva J-A, Jacobs IG, Frazer ARL, Jelinek GA. The association between hospital overcrowding and mortality among patients admitted via Western Australian emergency departments.[Erratum appears in Med J Aust. 2006 Jun 19;184(12):616]. Medical Journal of Australia. 2006;184(5):208–12. . - PubMed
-
- Richardson DB. Increase in patient mortality at 10 days associated with emergency department overcrowding. Medical Journal of Australia. 2006;184(5):213–6. . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
