

Camera-based photoplethysmography in an intraoperative setting
- PMID: 29540189
- PMCID: PMC5853087
- DOI: 10.1186/s12938-018-0467-7
Camera-based photoplethysmography in an intraoperative setting
Abstract
Background: Camera-based photoplethysmography (cbPPG) is a measurement technique which enables remote vital sign monitoring by using cameras. To obtain valid plethysmograms, proper regions of interest (ROIs) have to be selected in the video data. Most automated selection methods rely on specific spatial or temporal features limiting a broader application. In this work, we present a new method which overcomes those drawbacks and, therefore, allows cbPPG to be applied in an intraoperative environment.
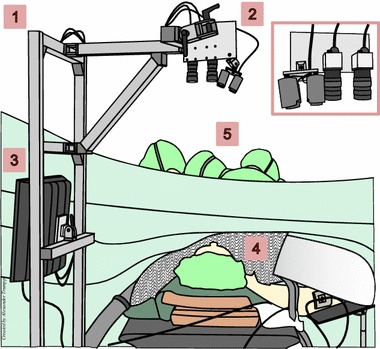
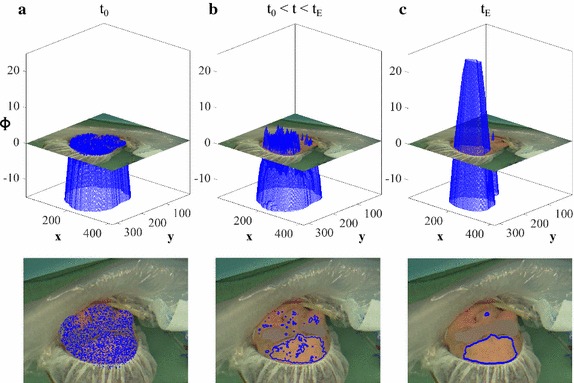
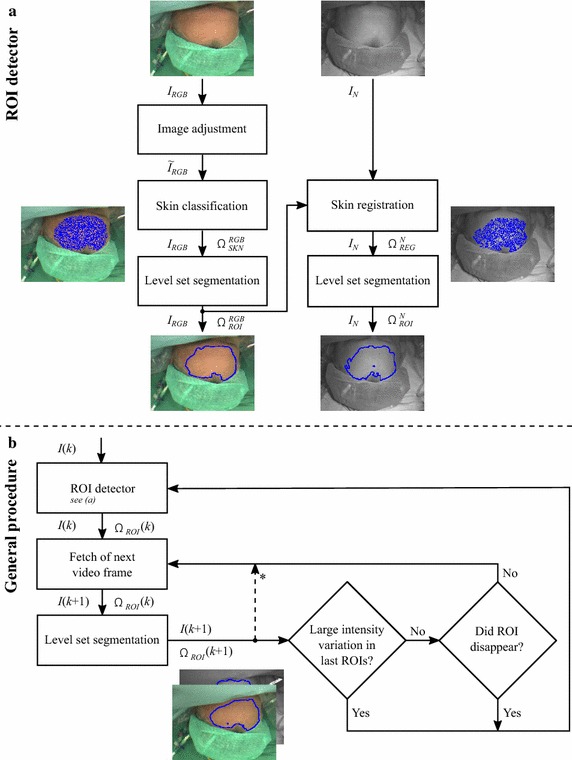
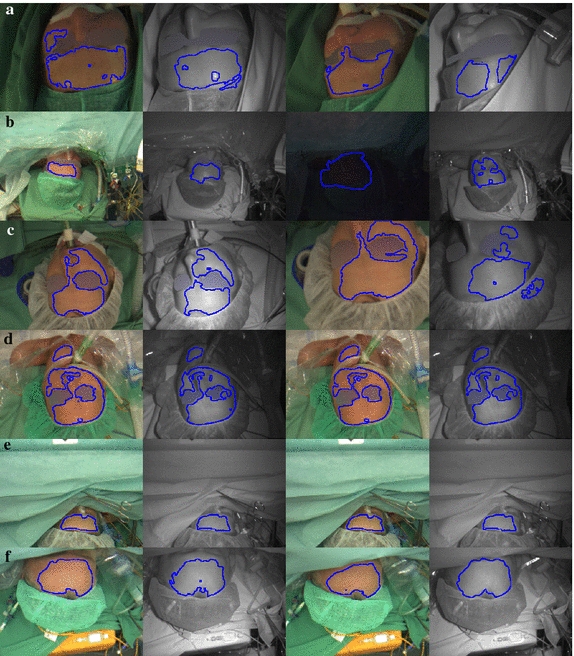
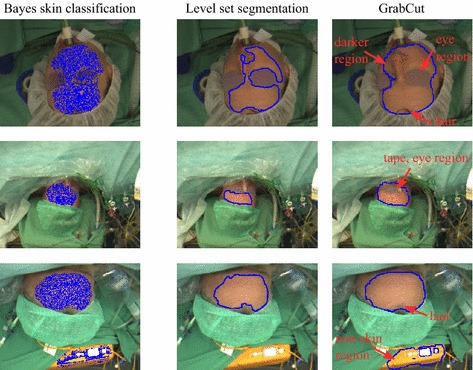
Methods: We recorded 41 patients during surgery using an RGB and a near-infrared (NIR) camera. A Bayesian skin classifier was employed to detect suitable regions, and a level set segmentation approach to define and track ROIs based on spatial homogeneity.
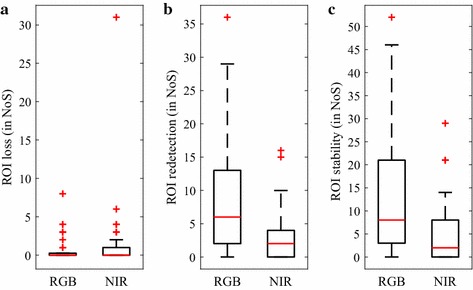
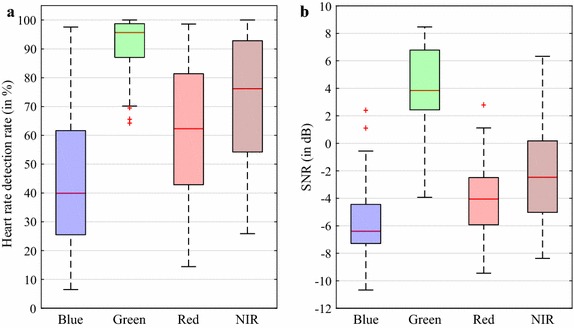
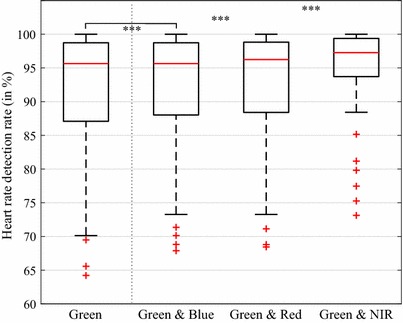
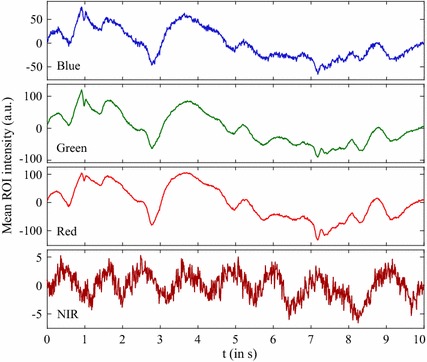
Results: The results show stable and homogeneously illuminated ROIs. We further evaluated their quality with regards to extracted cbPPG signals. The green channel provided the best results where heart rates could be correctly estimated in 95.6% of cases. The NIR channel yielded the highest contribution in compensating false estimations.
Conclusions: The proposed method proved that cbPPG is applicable in intraoperative environments. It can be easily transferred to other settings regardless of which body site is considered.
Keywords: Camera-based photoplethysmography; Intraoperative monitoring; Level set methods; Remote monitoring; Spatial homogeneity.
Figures
References
-
- Hülsbusch M, Blažek V. Contactless mapping of rhythmical phenomena in tissue perfusion using PPGI. In: Proceedings of SPIE, medical imaging 2002: physiology and function from multidimensional images, vol. 4683; 2002. p. 110–7.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
