

Pulmonary arterial hypertension: pathogenesis and clinical management
- PMID: 29540357
- PMCID: PMC6889979
- DOI: 10.1136/bmj.j5492
Pulmonary arterial hypertension: pathogenesis and clinical management
Abstract
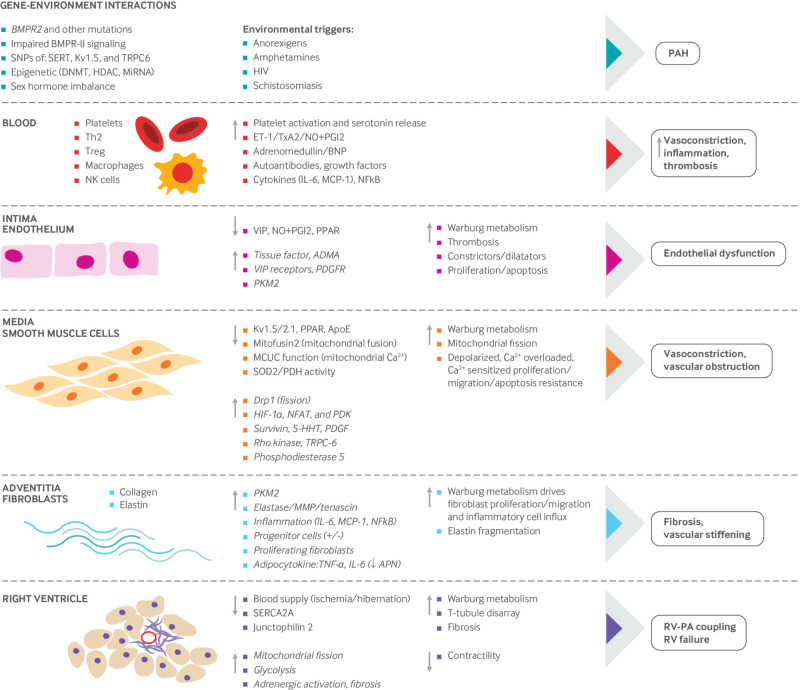
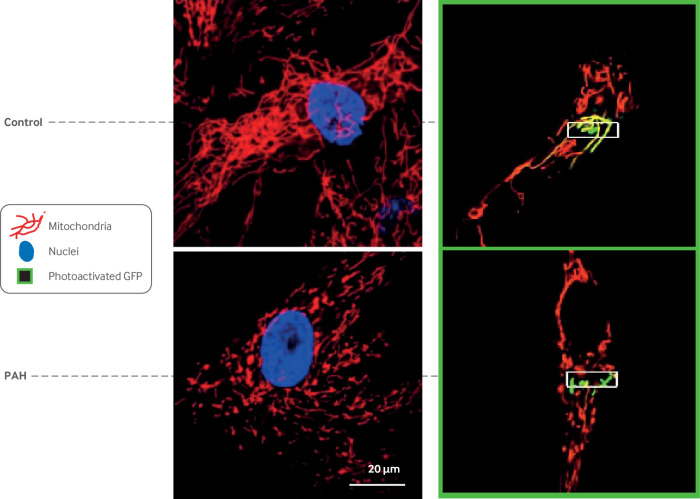
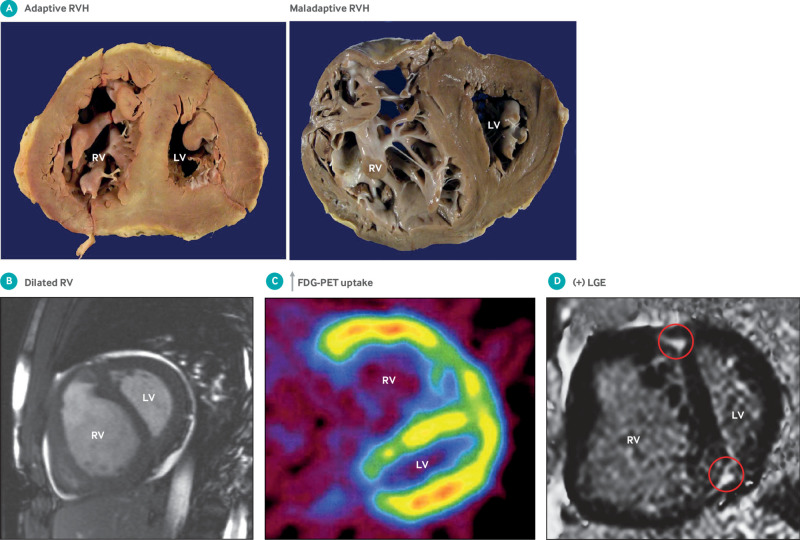
Pulmonary hypertension is defined as a resting mean pulmonary artery pressure of 25 mm Hg or above. This review deals with pulmonary arterial hypertension (PAH), a type of pulmonary hypertension that primarily affects the pulmonary vasculature. In PAH, the pulmonary vasculature is dynamically obstructed by vasoconstriction, structurally obstructed by adverse vascular remodeling, and pathologically non-compliant as a result of vascular fibrosis and stiffening. Many cell types are abnormal in PAH, including vascular cells (endothelial cells, smooth muscle cells, and fibroblasts) and inflammatory cells. Progress has been made in identifying the causes of PAH and approving new drug therapies. A cancer-like increase in cell proliferation and resistance to apoptosis reflects acquired abnormalities of mitochondrial metabolism and dynamics. Mutations in the type II bone morphogenetic protein receptor (BMPR2) gene dramatically increase the risk of developing heritable PAH. Epigenetic dysregulation of DNA methylation, histone acetylation, and microRNAs also contributes to disease pathogenesis. Aberrant bone morphogenetic protein signaling and epigenetic dysregulation in PAH promote cell proliferation in part through induction of a Warburg mitochondrial-metabolic state of uncoupled glycolysis. Complex changes in cytokines (interleukins and tumor necrosis factor), cellular immunity (T lymphocytes, natural killer cells, macrophages), and autoantibodies suggest that PAH is, in part, an autoimmune, inflammatory disease. Obstructive pulmonary vascular remodeling in PAH increases right ventricular afterload causing right ventricular hypertrophy. In some patients, maladaptive changes in the right ventricle, including ischemia and fibrosis, reduce right ventricular function and cause right ventricular failure. Patients with PAH have dyspnea, reduced exercise capacity, exertional syncope, and premature death from right ventricular failure. PAH targeted therapies (prostaglandins, phosphodiesterase-5 inhibitors, endothelin receptor antagonists, and soluble guanylate cyclase stimulators), used alone or in combination, improve functional capacity and hemodynamics and reduce hospital admissions. However, these vasodilators do not target key features of PAH pathogenesis and have not been shown to reduce mortality, which remains about 50% at five years. This review summarizes the epidemiology, pathogenesis, diagnosis, and treatment of PAH.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: We have read and understood the BMJ policy on declaration of interests and declare the following interests: TT received a modest honorarium from Gilead and Actelion for participating in an advisory board.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous