

Pseudomonas aeruginosa isolation in patients with non-cystic fibrosis bronchiectasis: a retrospective study
- PMID: 29540404
- PMCID: PMC5857665
- DOI: 10.1136/bmjopen-2016-014613
Pseudomonas aeruginosa isolation in patients with non-cystic fibrosis bronchiectasis: a retrospective study
Abstract
Objectives: Pseudomonas aeruginosa (P. aeruginosa) occupies an important niche in the pathogenic microbiome of bronchiectasis. The objective of this study is to evaluate the clinical characteristics and prognostic value of P. aeruginosa in Chinese adult patients with bronchiectasis.
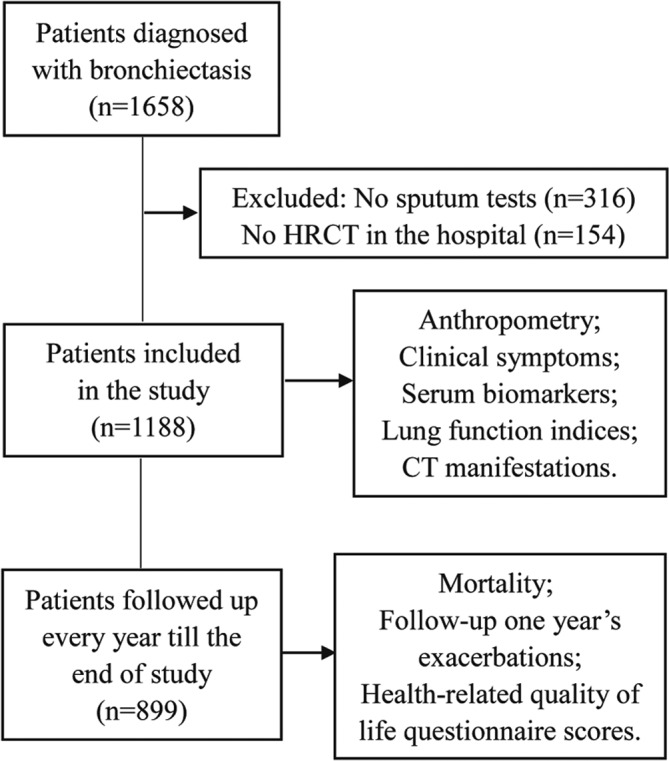
Methods: This retrospective and follow-up study enrolled 1188 patients diagnosed with bronchiectasis at Shanghai Pulmonary Hospital between January 2011 and December 2012. The patients' clinical data including anthropometry, clinical symptoms, serum biomarkers, radiographic manifestations and lung function indices were reviewed. The median follow-up duration (IQR) was 44 (40-54) months, during which 289 patients were lost to follow-up. Data from 899 patients were collected and analysed for the outcomes of mortality, annual exacerbation frequency and health-related quality of life.
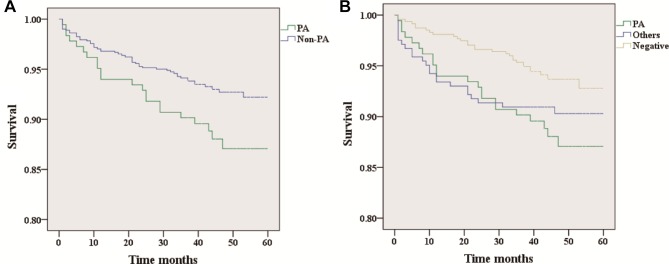
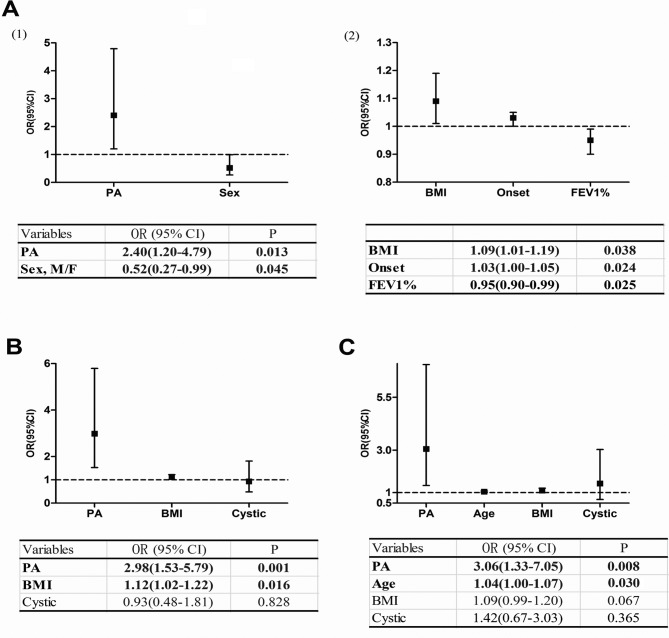
Results: P. aeruginosa was isolated from 232 patients, alongside other pathogens such as Aspergillus (n=75) and Candida albicans (n=72). There were 74 deaths (12% of patients with P. aeruginosa, 7.3% of those without) over the course of the follow-up. The isolation of P. aeruginosa was a risk factor for all-cause mortality (HR, 3.07; 95% CI 1.32 to 7.15) and was associated with high rates of exacerbations (ie, ≥3 exacerbations per year of follow-up) (HR, 2.40; 95% CI 1.20 to 4.79). Patients with P. aeruginosa also had worse scores on the Hospital Anxiety and Depression Scale (anxiety, p=0.005; depression, p<0.001), the Leicester Cough Questionnaire (p=0.033) and the modified Medical Research Council scale (p=0.001) compared with those without P. aeruginosa.
Conclusions: Isolation of P. aeruginosa in patients with bronchiectasis is a significant prognostic indicator and should be a major factor in the clinical management of the disease.
Keywords: bronchiectaiss; exacerbation; mortality; pseudomonas aeruginosa.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
The existence of bronchiectasis predicts worse prognosis in patients with COPD.Sci Rep. 2015 Jun 16;5:10961. doi: 10.1038/srep10961. Sci Rep. 2015. PMID: 26077673 Free PMC article.
-
Antibiotic-resistant Pseudomonas aeruginosa infection in patients with bronchiectasis: prevalence, risk factors and prognostic implications.Int J Chron Obstruct Pulmon Dis. 2018 Jan 9;13:237-246. doi: 10.2147/COPD.S150250. eCollection 2018. Int J Chron Obstruct Pulmon Dis. 2018. PMID: 29386892 Free PMC article.
-
Non cystic fibrosis bronchiectasis: A longitudinal retrospective observational cohort study of Pseudomonas persistence and resistance.Respir Med. 2015 Jun;109(6):716-26. doi: 10.1016/j.rmed.2014.07.021. Epub 2014 Aug 29. Respir Med. 2015. PMID: 25200914
-
A Comprehensive Analysis of the Impact of Pseudomonas aeruginosa Colonization on Prognosis in Adult Bronchiectasis.Ann Am Thorac Soc. 2015 Nov;12(11):1602-11. doi: 10.1513/AnnalsATS.201506-333OC. Ann Am Thorac Soc. 2015. PMID: 26356317 Review.
-
Chronic obstructive pulmonary disease and bronchiectasis.Curr Opin Pulm Med. 2013 Mar;19(2):133-9. doi: 10.1097/MCP.0b013e32835d8312. Curr Opin Pulm Med. 2013. PMID: 23287285 Review.
Cited by
-
Risk factors for Pseudomonas aeruginosa colonization in non-cystic fibrosis bronchiectasis and clinical implications.Respir Res. 2021 Apr 28;22(1):132. doi: 10.1186/s12931-021-01729-5. Respir Res. 2021. PMID: 33910573 Free PMC article.
-
Managing Bronchiectasis: 13 Years of Experience from Sputum to Lung Transplantation.Turk Thorac J. 2020 Jul;21(4):261-265. doi: 10.5152/TurkThoracJ.2019.19040. Turk Thorac J. 2020. PMID: 32687787 Free PMC article.
-
Tiotropium in Patients with Bronchiectasis: A Prospective Cohort Study.Lung. 2023 Feb;201(1):9-15. doi: 10.1007/s00408-023-00597-8. Epub 2023 Feb 7. Lung. 2023. PMID: 36746813
-
Bacteriophage: A new therapeutic player to combat neutrophilic inflammation in chronic airway diseases.Front Med (Lausanne). 2022 Dec 14;9:1069929. doi: 10.3389/fmed.2022.1069929. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36590945 Free PMC article. Review.
-
Cost-effectiveness analysis of two inhaled antibiotics for stable Bronchiectasis with Pseudomonas aeruginosa infections in China.PLoS One. 2025 Jun 18;20(6):e0324254. doi: 10.1371/journal.pone.0324254. eCollection 2025. PLoS One. 2025. PMID: 40531911 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical