

Is exercise-based cardiac rehabilitation effective? A systematic review and meta-analysis to re-examine the evidence
- PMID: 29540415
- PMCID: PMC5857699
- DOI: 10.1136/bmjopen-2017-019656
Is exercise-based cardiac rehabilitation effective? A systematic review and meta-analysis to re-examine the evidence
Erratum in
-
Correction: Is exercise-based cardiac rehabilitation effective? A systematic review and meta-analysis to re-examine the evidence.BMJ Open. 2018 May 14;8(5):e019656corr1. doi: 10.1136/bmjopen-2017-019656corr1. BMJ Open. 2018. PMID: 29764896 Free PMC article. No abstract available.
Abstract
Objectives: To determine the contemporary effectiveness of exercise-based cardiac rehabilitation (CR) in terms of all-cause mortality, cardiovascular mortality and hospital admissions.
Data sources: Studies included in or meeting the entry criteria for the 2016 Cochrane review of exercise-based CR in patients with coronary artery disease.
Study eligibility criteria: Randomised controlled trials (RCTs) of exercise-based CR versus a no-exercise control whose participants were recruited after the year 2000.
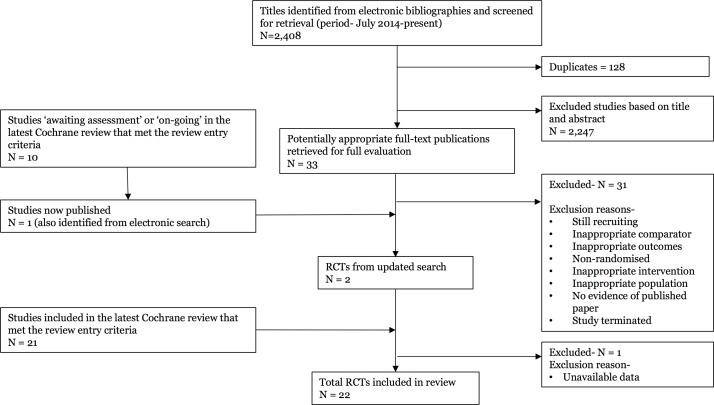
Study appraisal and synthesis methods: Two separate reviewers independently screened the characteristics of studies. One reviewer quality appraised any new studies and assessed their risk of bias using the Cochrane Collaboration's recommended risk of bias tool. Data were reported as the risk difference (95% CI).
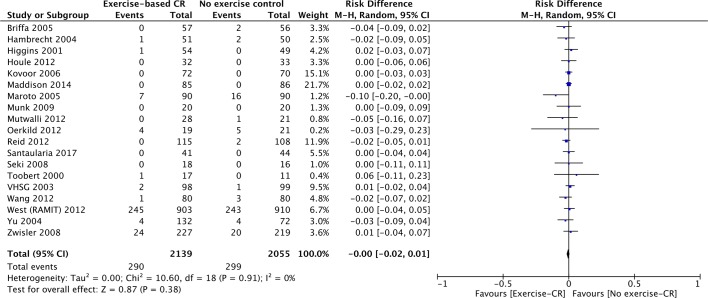
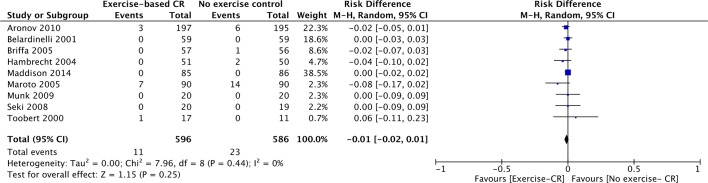
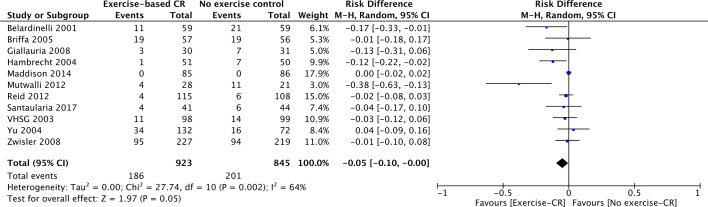
Results: We included 22 studies with 4834 participants (mean age 59.5 years, 78.4% male). We found no differences in outcomes between exercise-based CR and a no-exercise control at their longest follow-up period for: all-cause mortality (19 studies; n=4194; risk difference 0.00, 95% CI -0.02 to 0.01, P=0.38) or cardiovascular mortality (9 studies; n=1182; risk difference -0.01, 95% CI -0.02 to 0.01, P=0.25). We found a small reduction in hospital admissions of borderline statistical significance (11 studies; n=1768; risk difference -0.05, 95% CI -0.10 to -0.00, P=0.05).
Conclusions and implications of key findings: Our analysis indicates conclusively that the current approach to exercise-based CR has no effect on all-cause mortality or cardiovascular mortality, when compared with a no-exercise control. There may be a small reduction in hospital admissions following exercise-based CR that is unlikely to be clinically important.
Prospero registration number: CRD42017073616.
Keywords: all-cause mortality; cardiovascular mortality; coronary artery disease; exercise-based cardiac rehabilitation; hospital admissions..
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- World Health Organisation. Top 10 causes of death worldwide- Fact Sheet. 2017. http://www.who.int/mediacentre/factsheets/fs310/en/ (accessed 29 May 2017).
-
- NICE. Myocardial Infarction: cardiac rehabilitation and prevention of further cardiovascular disease. 2013. https://www.nice.org.uk/guidance/cg172/resources/myocardial-infarction-c... (accessed 31 May 2017).
-
- BACPR. Cardiovascular disease prevention and rehabilitation. 2012. http://www.bacpr.com/resources/46C_BACPR_Standards_and_Core_Components_2... (accessed 31 May 2017).
-
- Piepoli MF, Corrà U, Adamopoulos S, et al. Secondary prevention in the clinical management of patients with cardiovascular diseases. Core components, standards and outcome measures for referral and delivery: a policy statement from the cardiac rehabilitation section of the European association for cardiovascular prevention & rehabilitation. Endorsed by the committee for practice guidelines of the European society of cardiology. Eur J Prev Cardiol 2014;21:664–81. 10.1177/2047487312449597 - DOI - PubMed
-
- Balady GJ, Williams MA, Ades PA, et al. Core components of cardiac rehabilitation/secondary prevention programs: 2007 update: a scientific statement from the American heart association exercise, cardiac rehabilitation, and prevention committee, the council on clinical cardiology; the councils on cardiovascular nursing, epidemiology and prevention, and nutrition, physical activity, and metabolism; and the American association of cardiovascular and pulmonary rehabilitation. J Cardiopulm Rehabil Prev 2007;27:121–9. 10.1097/01.HCR.0000270696.01635.aa - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical