

Universal Genotyping for Tuberculosis Prevention Programs: a 5-Year Comparison with On-Request Genotyping
- PMID: 29540458
- PMCID: PMC5925716
- DOI: 10.1128/JCM.01778-17
Universal Genotyping for Tuberculosis Prevention Programs: a 5-Year Comparison with On-Request Genotyping
Abstract
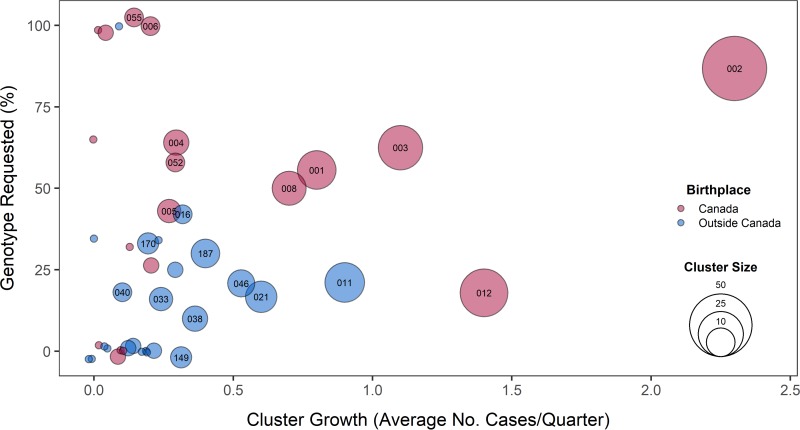
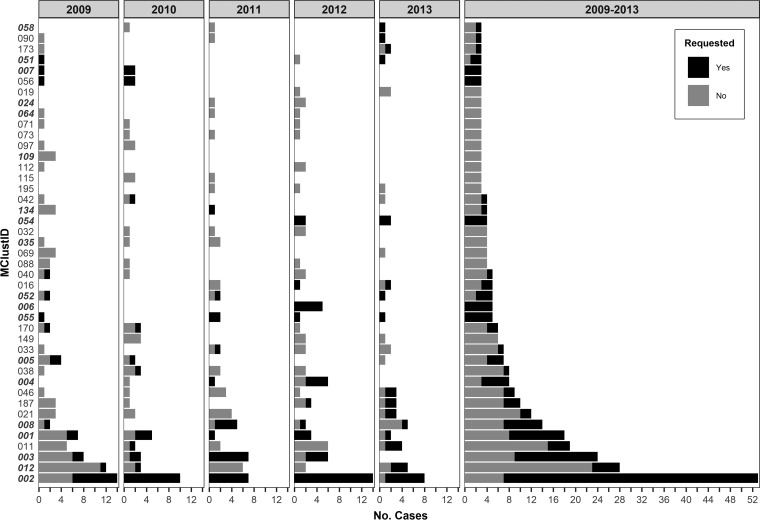
Prospective universal genotyping of tuberculosis (TB) isolates is used by many laboratories to detect clusters of cases and inform contact investigations. Prior to universal genotyping, most TB prevention programs genotyped isolates on request only, relying on requests from public health professionals whose knowledge of a patient's clinical, demographic, and epidemiological characteristics suggested potential transmission. To justify the switch from on-request to universal genotyping-particularly in the public health domain, with its limited resources and competing priorities-it is important to demonstrate the additional benefit provided by a universal genotyping program. We compared the clustering patterns revealed by retrospective 24-locus mycobacterial interspersed repetitive unit-variable-number tandem repeat genotyping of all culture-positive isolates over a 5-year period to the patterns previously established by our genotyping-on-request program in the low-incidence setting of British Columbia, Canada. We found that 23.8% of isolates were requested during the study period, and while requested isolates had increased odds of belonging to a genotype cluster (adjusted odds ratio, 2.3; 95% confidence interval, 1.5 to 3.3), only 54.6% clustered with the requested comparator strain. Universal genotyping revealed 94 clusters ranging in size from 2 to 53 isolates (mean = 5) and involving 432 individuals. On-request genotyping missed 54 (57.4%) of these clusters and 130 (30.1%) clustered individuals. Our results underscore that TB patient networks are complex, with unrecognized linkages between patients, and a prospective province-wide universal genotyping program provides an informative, bias-free tool to explore transmission to a degree not possible with on-request genotyping.
Keywords: MIRU-VNTR genotyping; program assessment; tuberculosis.
Copyright © 2018 Guthrie et al.
Figures
Similar articles
-
Prospective universal application of mycobacterial interspersed repetitive-unit-variable-number tandem-repeat genotyping to characterize Mycobacterium tuberculosis isolates for fast identification of clustered and orphan cases.J Clin Microbiol. 2009 Jul;47(7):2026-32. doi: 10.1128/JCM.02308-08. Epub 2009 May 20. J Clin Microbiol. 2009. PMID: 19458183 Free PMC article.
-
Assessment of an optimized mycobacterial interspersed repetitive- unit-variable-number tandem-repeat typing system combined with spoligotyping for population-based molecular epidemiology studies of tuberculosis.J Clin Microbiol. 2007 Mar;45(3):691-7. doi: 10.1128/JCM.01393-06. Epub 2006 Dec 27. J Clin Microbiol. 2007. PMID: 17192416 Free PMC article.
-
Sensitivities and specificities of spoligotyping and mycobacterial interspersed repetitive unit-variable-number tandem repeat typing methods for studying molecular epidemiology of tuberculosis.J Clin Microbiol. 2005 Jan;43(1):89-94. doi: 10.1128/JCM.43.1.89-94.2005. J Clin Microbiol. 2005. PMID: 15634955 Free PMC article.
-
[New era in molecular epidemiology of tuberculosis in Japan].Kekkaku. 2006 Nov;81(11):693-707. Kekkaku. 2006. PMID: 17154049 Review. Japanese.
-
The Ontario universal typing of tuberculosis (OUT-TB) surveillance program--what it means to you.Can Respir J. 2010 May-Jun;17(3):e51-4. doi: 10.1155/2010/715202. Can Respir J. 2010. PMID: 20617215 Free PMC article. Review.
Cited by
-
Genotyped cluster investigations versus standard contact tracing: comparative impact on latent tuberculosis infection cascade of care in a low-incidence region.BMC Infect Dis. 2025 Jan 16;25(1):74. doi: 10.1186/s12879-024-10358-4. BMC Infect Dis. 2025. PMID: 39819477 Free PMC article.
-
Complexities and benefits of adopting next-generation sequencing-based tuberculosis diagnostics: a qualitative study among stakeholders in low and high-income countries.BMJ Open. 2023 Apr 10;13(4):e066651. doi: 10.1136/bmjopen-2022-066651. BMJ Open. 2023. PMID: 37037623 Free PMC article.
-
Immunoinformatics and Vaccine Development: An Overview.Immunotargets Ther. 2020 Feb 26;9:13-30. doi: 10.2147/ITT.S241064. eCollection 2020. Immunotargets Ther. 2020. PMID: 32161726 Free PMC article. Review.
-
Characterization of Mycobacterium tuberculosis strains in Beijing, China: drug susceptibility phenotypes and Beijing genotype family transmission.BMC Infect Dis. 2018 Dec 14;18(1):658. doi: 10.1186/s12879-018-3578-7. BMC Infect Dis. 2018. PMID: 30547765 Free PMC article.
-
TB Transmission: Closing the Gaps.EBioMedicine. 2018 Aug;34:4-5. doi: 10.1016/j.ebiom.2018.07.020. Epub 2018 Jul 30. EBioMedicine. 2018. PMID: 30072212 Free PMC article. No abstract available.
References
-
- Lönnroth K, Migliori GB, Abubakar I, D'Ambrosio L, de Vries G, Diel R, Douglas P, Falzon D, Gaudreau M-A, Goletti D, González Ochoa ER, LoBue P, Matteelli A, Njoo H, Solovic I, Story A, Tayeb T, van der Werf MJ, Weil D, Zellweger J-P, Abdel Aziz M, Al Lawati MRM, Aliberti S, Arrazola de Oñate W, Barreira D, Bhatia V, Blasi F, Bloom A, Bruchfeld J, Castelli F, Centis R, Chemtob D, Cirillo DM, Colorado A, Dadu A, Dahle UR, De Paoli L, Dias HM, Duarte R, Fattorini L, Gaga M, Getahun H, Glaziou P, Goguadze L, Del Granado M, Haas W, Järvinen A, Kwon G-Y, Mosca D, Nahid P, et al. . 2015. Towards tuberculosis elimination: an action framework for low-incidence countries. Eur Respir J 45:928–952. doi:10.1183/09031936.00214014. - DOI - PMC - PubMed
-
- Public Health Agency of Canada. 2014. Canadian tuberculosis standards 7th edition: 2014. Public Health Agency of Canada, Ottawa, Ontario, Canada: https://www.canada.ca/en/public-health/services/infectious-diseases/cana....
-
- Gardy JL, Johnston JC, Ho Sui SJ, Cook VJ, Shah L, Brodkin E, Rempel S, Moore R, Zhao Y, Holt R, Varhol R, Birol I, Lem M, Sharma MK, Elwood K, Jones SJM, Brinkman FSL, Brunham RC, Tang P. 2011. Whole-genome sequencing and social-network analysis of a tuberculosis outbreak. N Engl J Med 364:730–739. doi:10.1056/NEJMoa1003176. - DOI - PubMed
-
- Adam HJ, Guthrie JL, Bolotin S, Alexander DC, Stuart R, Pyskir D, Brown EM, Rea E, Chedore P, Jamieson FB. 2010. Genotypic characterization of tuberculosis transmission within Toronto's under-housed population, 1997–2008. Int J Tuberc Lung Dis 14:1350–1353. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
