

Global Incidence and mortality of oesophageal cancer and their correlation with socioeconomic indicators temporal patterns and trends in 41 countries
- PMID: 29540708
- PMCID: PMC5852053
- DOI: 10.1038/s41598-018-19819-8
Global Incidence and mortality of oesophageal cancer and their correlation with socioeconomic indicators temporal patterns and trends in 41 countries
Abstract
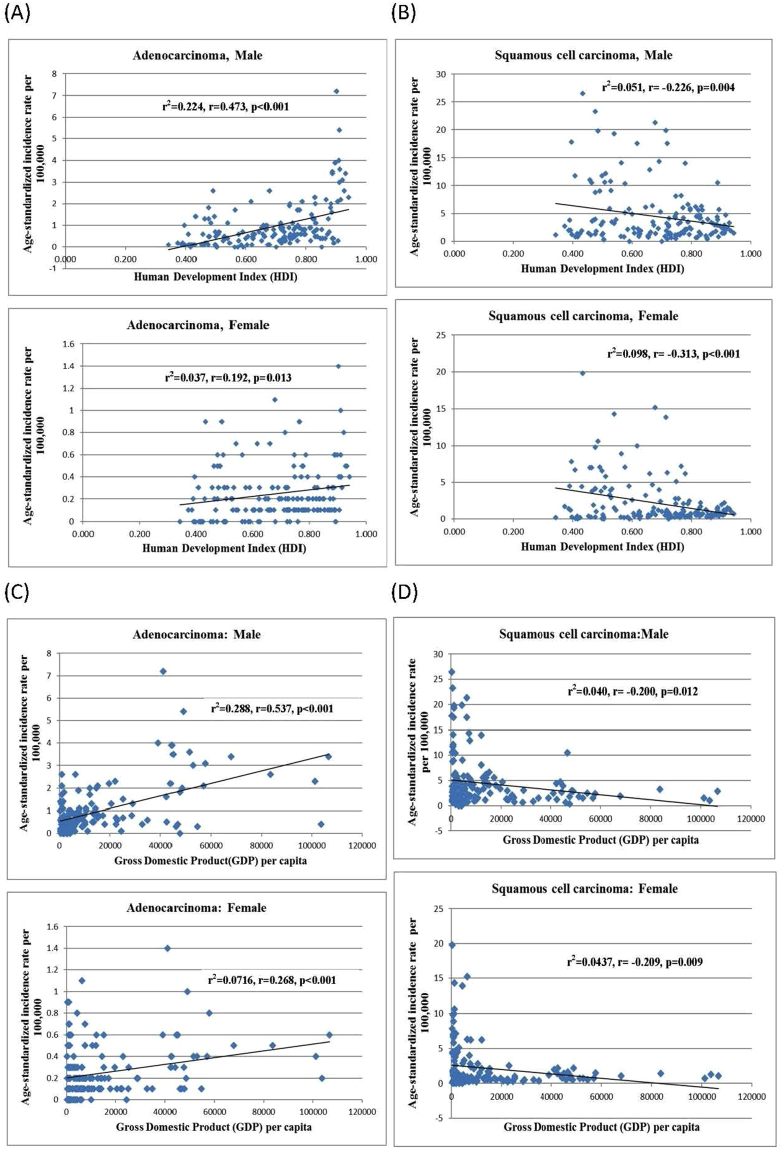
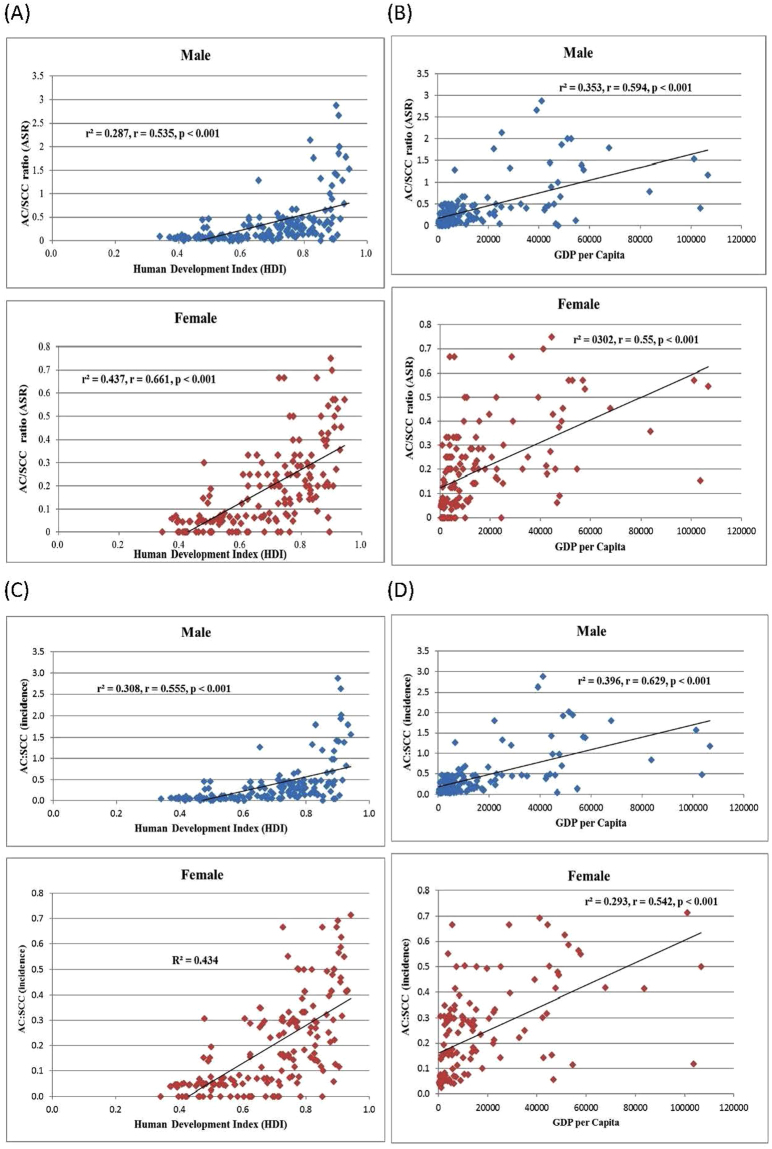
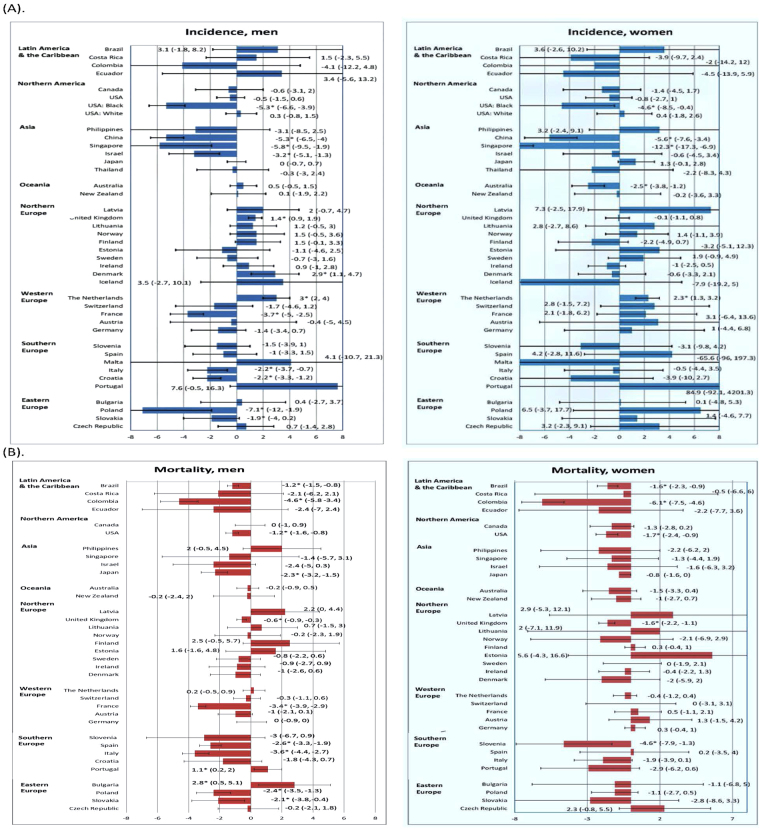
Oesophageal cancers (adenocarcinomas [AC] and squamous cell carcinomas [SCC]) are characterized by high incidence/mortality in many countries. We aimed to delineate its global incidence and mortality, and studied whether socioeconomic development and its incidence rate were correlated. The age-standardized rates (ASRs) of incidence and mortality of this medical condition in 2012 for 184 nations from the GLOBOCAN database; national databases capturing incidence rates, and the WHO mortality database were examined. Their correlations with two indicators of socioeconomic development were evaluated. Joinpoint regression analysis was used to generate trends. The ratio between the ASR of AC and SCC was strongly correlated with HDI (r = 0.535 [men]; r = 0.661 [women]) and GDP (r = 0.594 [men]; r = 0.550 [women], both p < 0.001). Countries that reported the largest reduction in incidence in male included Poland (Average Annual Percent Change [AAPC] = -7.1, 95%C.I. = -12,-1.9) and Singapore (AAPC = -5.8, 95%C.I. = -9.5,-1.9), whereas for women the greatest decline was seen in Singapore (AAPC = -12.3, 95%C.I. = -17.3,-6.9) and China (AAPC = -5.6, 95%C.I. = -7.6,-3.4). The Philippines (AAPC = 4.3, 95%C.I. = 2,6.6) and Bulgaria (AAPC = 2.8, 95%C.I. = 0.5,5.1) had a significant mortality increase in men; whilst Columbia (AAPC = -6.1, 95%C.I. = -7.5,-4.6) and Slovenia (AAPC = -4.6, 95%C.I. = -7.9,-1.3) reported mortality decline in women. These findings inform individuals at increased risk for primary prevention.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Ferlay, J., Soerjomataram, I. & Ervik, M. et al. GLOBOCAN 2012v1.0, Cancer Incidence and Mortality Worldwide. IARC Cancer Base No. 11. Lyon, France: International Agency for Research on Cancer (2013).
-
- Mao WM, Zheng WH, Long ZQ. Epidemiologic risk factors for esophageal cancer development. Asian Pac J Cancer Prev. 2011;12:2461–2466. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
