

Using the Oxford Cognitive Screen to Detect Cognitive Impairment in Stroke Patients: A Comparison with the Mini-Mental State Examination
- PMID: 29541055
- PMCID: PMC5836594
- DOI: 10.3389/fneur.2018.00101
Using the Oxford Cognitive Screen to Detect Cognitive Impairment in Stroke Patients: A Comparison with the Mini-Mental State Examination
Abstract
Background: The Oxford Cognitive Screen (OCS) was recently developed with the aim of describing the cognitive deficits after stroke. The scale consists of 10 tasks encompassing five cognitive domains: attention and executive function, language, memory, number processing, and praxis. OCS was devised to be inclusive and un-confounded by aphasia and neglect. As such, it may have a greater potential to be informative on stroke cognitive deficits of widely used instruments, such as the Mini-Mental State Examination (MMSE) or the Montreal Cognitive Assessment, which were originally devised for demented patients.
Objective: The present study compared the OCS with the MMSE with regards to their ability to detect cognitive impairments post-stroke. We further aimed to examine performance on the OCS as a function of subtypes of cerebral infarction and clinical severity.
Methods: 325 first stroke patients were consecutively enrolled in the study over a 9-month period. The OCS and MMSE, as well as the Bamford classification and NIHSS, were given according to standard procedures.
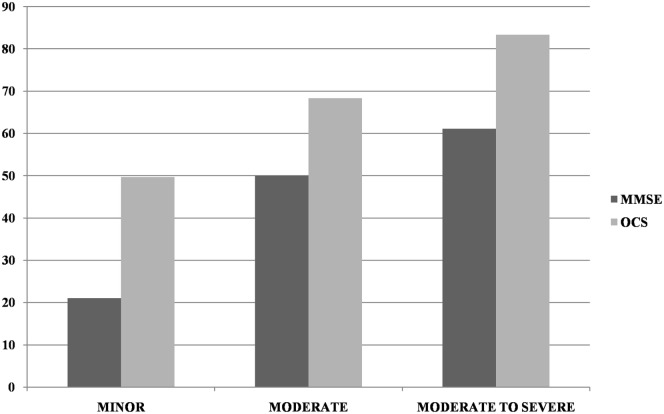
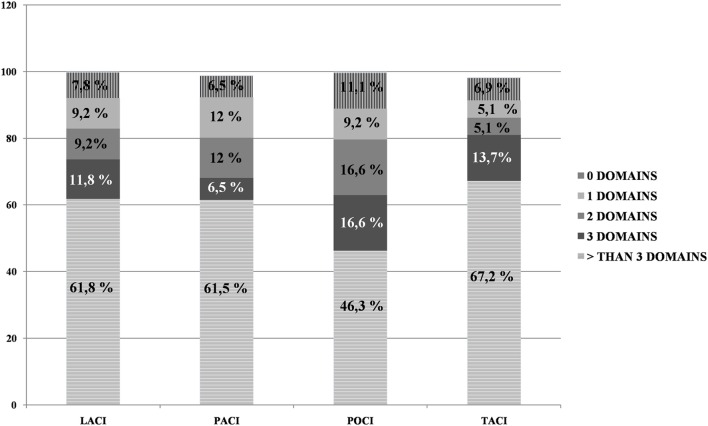
Results: About a third of patients (35.3%) had a performance lower than the cutoff (<22) on the MMSE, whereas 91.6% were impaired in at least one OCS domain, indicating higher incidences of impairment for the OCS. More than 80% of patients showed an impairment in two or more cognitive domains of the OCS. Using the MMSE as a standard of clinical practice, the comparative sensitivity of OCS was 100%. Out of the 208 patients with normal MMSE performance 180 showed impaired performance in at least one domain of the OCS. The discrepancy between OCS and MMSE was particularly strong for patients with milder strokes. As for subtypes of cerebral infarction, fewer patients demonstrated widespread impairments in the OCS in the Posterior Circulation Infarcts category than in the other categories.
Conclusion: Overall, the results showed a much higher incidence of cognitive impairment with the OCS than with the MMSE and demonstrated no false negatives for OCS vs MMSE. It is concluded that OCS is a sensitive screen tool for cognitive deficits after stroke. In particular, the OCS detects high incidences of stroke-specific cognitive impairments, not detected by the MMSE, demonstrating the importance of cognitive profiling.
Keywords: Mini-Mental State Examination; Oxford Cognitive Screen; cognitive assessment; cognitive screening; stroke.
Figures
References
-
- SPREAD. Stroke Prevention and Educational Awareness Diffusion. 8th ed (2017). AN: L.T.COM.09.2016.1690 cod. Art. 86145856.
-
- Liman TG, Heuschmann PU, Endres M, Floel A, Schwab S, Kolominsky-Rabas PL. Changes in cognitive function over 3 years after first-ever stroke and predictors of cognitive impairment and long-term cognitive stability: the Erlangen Stroke Project. Dement Geriatr Cogn Disord (2011) 31:291–9. 10.1159/000327358 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials