

Oncological safety of nipple-sparing mastectomy in young patients with breast cancer compared with conventional mastectomy
- PMID: 29541245
- PMCID: PMC5835917
- DOI: 10.3892/ol.2018.7913
Oncological safety of nipple-sparing mastectomy in young patients with breast cancer compared with conventional mastectomy
Abstract
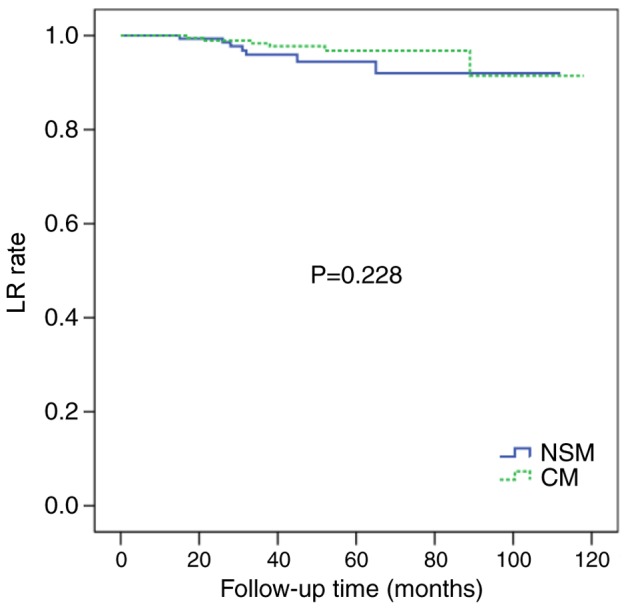
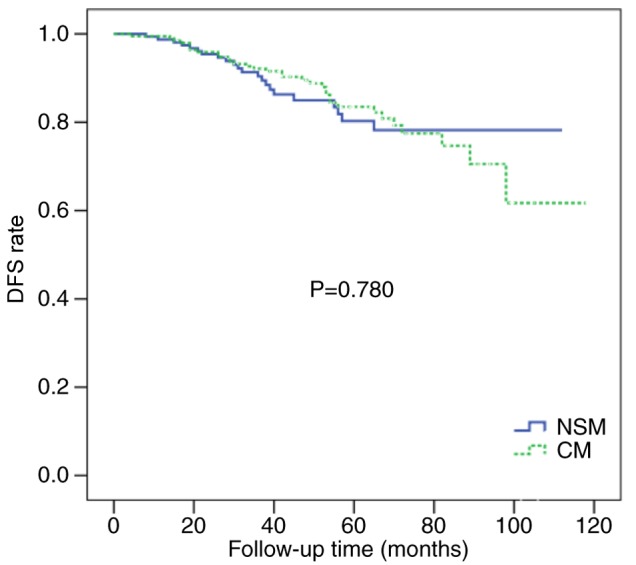
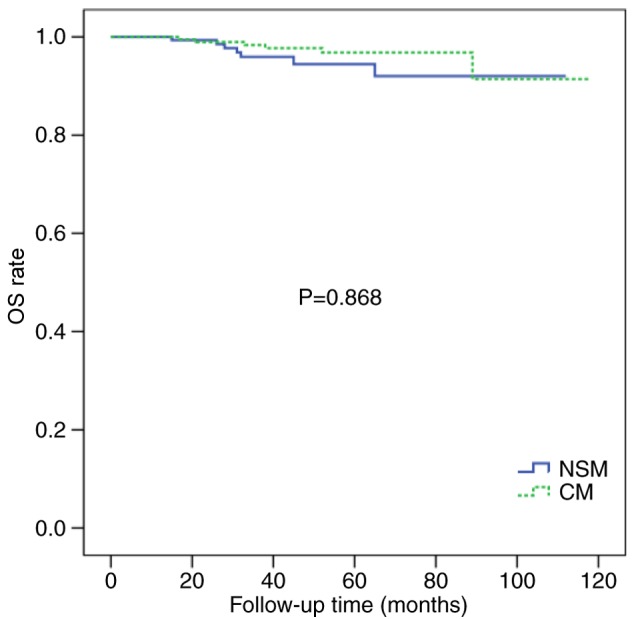
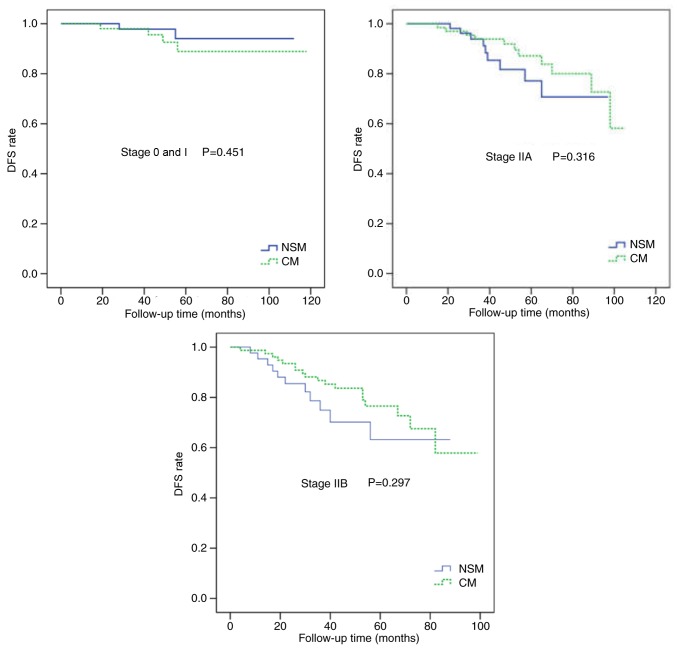
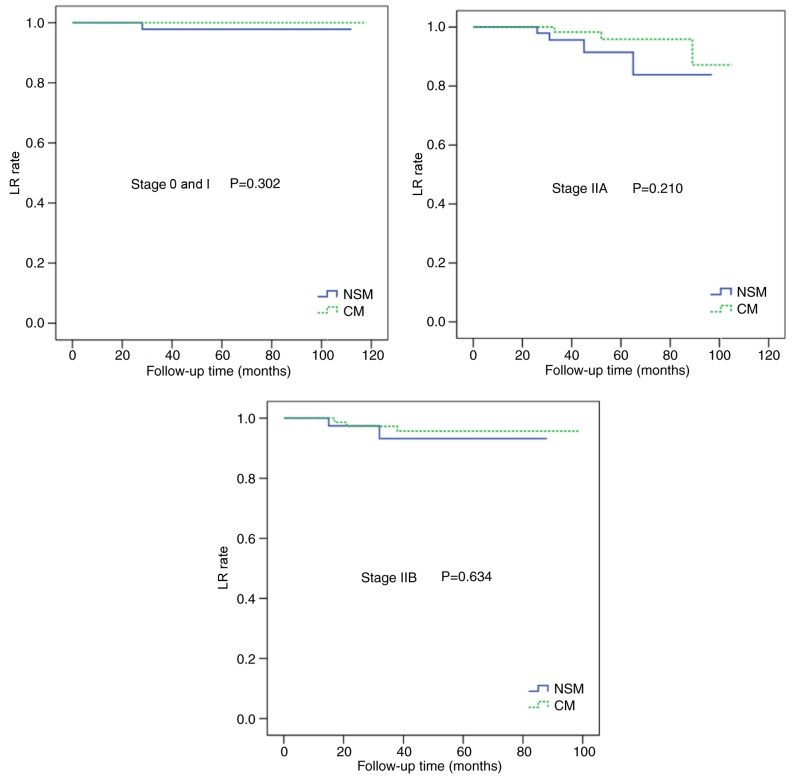
Although nipple-sparing mastectomy (NSM) is being used more frequently, the oncological safety of NSM remains unclear, particularly in young patients (<35 years). The aim of the present study was to compare the rates of local recurrence (LR), disease-free survival (DFS) and overall survival (OS) in young patients with breast cancer who had undergone NSM or conventional mastectomy (CM). The clinicopathological data of young patients with stage 0-IIB breast cancer who had undergone NSM (163 cases) or CM (194 cases) between 2007 and 2016 were retrospectively analyzed. The log-rank test was used to analyze the differences in the LR, DFS and OS rates between the two groups and multivariate analysis was used to analyze the patient prognostic factors for DFS. The median follow-up time was 49 months. Patients who had undergone CM were more likely to exhibit stage II disease (68.4 vs. 58.3%; P=0.015) and positive lymph nodes (45.9 vs. 33.1%; P=0.014). In the NSM group, LR occurred in 7 (4.3%) cases, systemic recurrence in 15 (9.2%) cases and mortality in 9 (5.5%) cases. In the CM group, LR occurred in 6 (3.1%) cases, systemic recurrence in 27 (13.9%) cases and mortality in 15 (7.7%) cases. There were no statistical differences in the LR, DFS and OS rates between the two groups (P>0.05). Following adjustment for clinical stage, the LR and DFS rates between the two groups exhibited no significant differences. Analysis of the prognostic factors demonstrated that clinical stage, lymph node status, estrogen and progesterone receptor status and human epidermal growth factor receptor 2 status were associated with DFS (P<0.05). NSM is safe for young patients with early-stage breast cancer and provides patients with an improved cosmetic outcome. Furthermore, nipple-areola complex preservation does not increase the risk of recurrence.
Keywords: breast cancer; early stage; nipple-sparing mastectomy; oncological safety; prognosis; young patient.
Figures
Similar articles
-
[Oncological safety and prognosis factors analysis of immediate breast reconstruction after nipple-areola-complex sparing mastectomy].Zhonghua Zhong Liu Za Zhi. 2018 Sep 23;40(9):690-695. doi: 10.3760/cma.j.issn.0253-3766.2018.09.011. Zhonghua Zhong Liu Za Zhi. 2018. PMID: 30293396 Chinese.
-
Initial oncological outcomes of nipple- and areola-sparing mastectomy in patients with breast cancer with nipple discharge.World J Surg Oncol. 2025 Apr 11;23(1):137. doi: 10.1186/s12957-025-03792-4. World J Surg Oncol. 2025. PMID: 40217492 Free PMC article.
-
A Propensity Score-matched Analysis of Long-term Oncologic Outcomes After Nipple-sparing Versus Conventional Mastectomy for Locally Advanced Breast Cancer.Ann Surg. 2022 Aug 1;276(2):386-390. doi: 10.1097/SLA.0000000000004416. Epub 2020 Nov 18. Ann Surg. 2022. PMID: 33201107
-
Local recurrence of mammary Paget's disease after nipple-sparing mastectomy and implant breast reconstruction: a case report and literature review.World J Surg Oncol. 2022 Sep 6;20(1):285. doi: 10.1186/s12957-022-02746-4. World J Surg Oncol. 2022. PMID: 36064544 Free PMC article. Review.
-
Defining a place for nipple sparing mastectomy in modern breast care: an evidence based review.Breast J. 2013 Nov-Dec;19(6):571-81. doi: 10.1111/j.1524-4741.2011.01220.x. Epub 2012 Jan 29. Breast J. 2013. PMID: 22284266 Review.
Cited by
-
Long-term outcomes of skin-sparing mastectomy and nipple-sparing mastectomy versus traditional mastectomy in breast cancer: a case-control study based on preoperative ultrasound and clinical indicators.World J Surg Oncol. 2025 Feb 14;23(1):52. doi: 10.1186/s12957-025-03695-4. World J Surg Oncol. 2025. PMID: 39953494 Free PMC article.
-
Postmastectomy Breast Reconstruction in Patients with Non-Metastatic Breast Cancer: A Systematic Review.Curr Oncol. 2025 Apr 16;32(4):231. doi: 10.3390/curroncol32040231. Curr Oncol. 2025. PMID: 40277787 Free PMC article.
-
Expert consensus on diagnosis, treatment and fertility management of young breast cancer patients.J Natl Cancer Cent. 2021 Feb 25;1(1):23-30. doi: 10.1016/j.jncc.2021.02.001. eCollection 2021 Mar. J Natl Cancer Cent. 2021. PMID: 39036789 Free PMC article.
-
Nipple-sparing mastectomy in young versus elderly patients.Rev Bras Ginecol Obstet. 2024 Oct 23;46:e-rbgo90. doi: 10.61622/rbgo/2024rbgo90. eCollection 2024. Rev Bras Ginecol Obstet. 2024. PMID: 39530073 Free PMC article.
References
-
- Madden JL. Modified radical mastectomy. Surg Gynecol Obstet. 1965;121:1221–1230. - PubMed
-
- Clarke M, Collins R, Darby S, Davies C, Elphinstone P, Evans V, Godwin J, Gray R, Hicks C, James S, et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: An overview of the randomised trials. Lancet. 2005;366:2087–2106. doi: 10.1016/S0140-6736(05)67887-7. - DOI - PubMed
-
- Fisher B, Anderson S, Redmond CK, Wolmark N, Wickerham DL, Cronin WM. Reanalysis and results after 12 years of follow-up in a randomized clinical trial comparing total mastectomy with lumpectomy with or without irradiation in the treatment of breast cancer. N Engl J Med. 1995;333:1456–1461. doi: 10.1056/NEJM199511303332203. - DOI - PubMed
-
- Voogd AC, Nielsen M, Peterse JL, Blichert-Toft M, Bartelink H, Overgaard M, van Tienhoven G, Andersen KW, Sylvester RJ, van Dongen JA, Danish Breast Cancer Cooperative Group. Breast Cancer Cooperative Group of the European Organization for Research and Treatment of Cancer Differences in risk factors for local and distant recurrence after breast-conserving therapy or mastectomy for stage I and II breast cancer: Pooled results of two large European randomized trials. J Clin Oncol. 2001;19:1688–1697. doi: 10.1200/JCO.2001.19.6.1688. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials